

Vitamins micronutrient compounds are essential organic molecules required in small amounts for proper physiological functioning. Despite their minuscule quantities, these compounds play crucial roles in energy production, immune function, bone development, and muscle tissue repair.
The human body cannot produce most vitamins or synthesise them in insufficient amounts, so dietary intake is necessary for optimal health.
These bioactive substances (naturally occurring compounds that affect living tissue) participate in numerous enzymatic reactions, serving as coenzymes (helper molecules) or cofactors (non-protein chemical compounds) that facilitate metabolic (energy-producing) processes. For instance, B vitamins contribute to energy metabolism by converting dietary energy into adenosine triphosphate (ATP), the primary energy currency of cells.
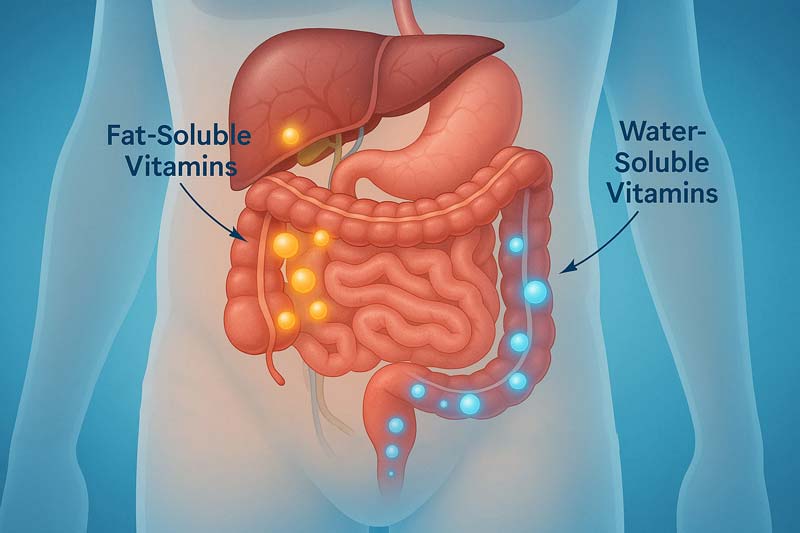
Meanwhile, antioxidant vitamins (compounds that neutralise harmful free radicals) such as C and E protect cells from oxidative damage caused by free radicals. Vitamins are categorised into fat-soluble (A, D, E, K) and water-soluble (B-complex, C) groups, reflecting their absorption mechanisms and storage capacities.
Fat-soluble vitamins dissolve in dietary fat and can be stored in the body’s tissues. In contrast, water-soluble vitamins dissolve in water and require more frequent consumption as excess amounts are excreted.
In the following sections, we’ll explore the classification and functions of vitamins micronutrient elements, examine factors affecting their absorption, present a comprehensive reference guide, discuss deficiency and toxicity considerations, and trace the historical evolution of our understanding of these vital compounds. This journey through vitamin science will provide insights into why these minuscule nutrients significantly impact human health.
Essential Vitamins Micronutrient Classification and Their Roles
Vitamins micronutrient compounds fall into two categories based on their solubility characteristics, influencing how they’re absorbed, transported, and stored in the body.
| Fat-Soluble Vitamins | Water-Soluble Vitamins |
|---|---|
| Dissolve in dietary fats | Dissolve in water |
| Stored in liver and fatty tissues | Generally not stored (except B12) |
| Require bile acids for absorption | Absorbed directly into bloodstream |
| Include vitamins A, D, E, K | Include B-complex vitamins and vitamin C |
| Excess amounts can accumulate | Excess typically excreted in urine |
Fat-soluble vitamins and micronutrient elements serve specialised bodily functions, as shown in the table above. Vitamin A maintains vision, immune function, reproduction, and cellular differentiation. Vitamin D regulates calcium and phosphorus absorption for bone health. Vitamin E is an antioxidant, protecting cell membranes and supporting immune function. Vitamin K is a cofactor for blood coagulation (the process of blood clot formation), bone metabolism, and vascular health.
Water-soluble vitamins perform equally vital roles. B-complex vitamins (B1, B2, B3, B6, B12, folate, biotin, and pantothenic acid) are central to energy metabolism and support red blood cell formation and nervous system function.
Vitamin C contributes to collagen (a protein providing structure to skin, bones, and connective tissues) synthesis for tissue repair and provides antioxidant protection.
Primary Biological Functions by System:
- Nervous System – B vitamins maintain nerve cell function and myelin sheath formation (protective coating around nerves). Vitamin B1 (thiamin) supports nerve impulse transmission, while B12 is essential for neurological health.
- Musculoskeletal System – Vitamin D enables calcium absorption for bone development, whilst vitamin K activates proteins needed for bone mineralisation (hardening of bone tissue). Vitamin C facilitates collagen formation required for joint and connective tissue health.
- Immune Function – Vitamins A, C, D, and E enhance innate and adaptive immune responses. Vitamin A maintains mucous membrane integrity, whilst vitamin D helps regulate immune cell development and function.
- Cardiovascular Health – B vitamins (particularly B6, B12, and folate) help metabolise homocysteine (an amino acid, a building block of protein) linked to heart disease when elevated. Vitamin E protects against oxidative damage in blood vessels.
- Vision – Vitamin A is crucial for maintaining the light-sensing cells in the retina. Beta-carotene (a plant pigment that converts to vitamin A), a precursor, and vitamins C and E help protect eye tissues from oxidative stress.
The interaction between vitamins micronutrient compounds demonstrates the sophistication of human metabolism. For instance, vitamin E regenerates vitamin C after it neutralises free radicals, showing how these nutrients work synergistically rather than in isolation.
Absorption Factors and Bioavailability
The absorption and utilisation of vitamins micronutrient compounds involve sophisticated processes that depend on various physiological factors. Examining these mechanisms helps explain why consuming vitamins doesn’t guarantee their effective use by the body.
Let’s explore the absorption journey of vitamins from consumption to utilisation:
1: Initial Uptake Factors
The chemical nature of vitamins micronutrient elements significantly influences their absorption pathways. Fat-soluble vitamins (A, D, E, K) require dietary fat for efficient absorption. Without adequate fat consumption, these vitamins pass through the digestive system largely unutilised.
For instance, vitamin E absorption can be as low as 10% without fat present, whilst proper fat consumption increases absorption to nearly 60%. Water-soluble vitamins follow different absorption patterns. B vitamins and vitamin C dissolve readily in the watery environment of the digestive tract and absorb directly into the bloodstream. However, they face their own challenges, such as competition for specialised transporters in the intestines.
2: Transport Mechanisms
After absorption, vitamins must be transported to their sites of action. Fat-soluble vitamins incorporate into chylomicrons (fat-protein particles) and travel through the lymphatic system (network of vessels carrying fluid, nutrients, and waste) before entering the bloodstream.
Water-soluble vitamins enter the portal circulation directly for transport to the liver. Specific carrier proteins facilitate vitamin movement throughout the body. Vitamin A requires retinol-binding protein (a transport protein for vitamin A), whilst vitamin D relies on vitamin D-binding protein.
These transport proteins ensure vitamins reach their target tissues and protect against premature excretion.
3: Bioavailability Modifiers
Several factors can enhance or impair vitamins micronutrient bioavailability (the proportion of a nutrient that is absorbed and used by the body):
- Dietary Matrix Effects – The food environment affects vitamin accessibility. For example, folate from food sources is approximately 50% bioavailable, whereas synthetic folic acid in supplements exhibits 85% bioavailability.
- Nutrient Interactions – Vitamins and minerals interact in ways that affect each other’s absorption. Vitamin C enhances iron absorption, whilst excessive zinc can impair copper uptake. Vitamin D and magnesium work together; magnesium is essential for vitamin D metabolism.
- Physiological Factors – Age influences absorption capacity, particularly for vitamin B12, which requires intrinsic factors produced in the stomach. As people age, their ability to produce inherent factors often diminishes, leading to decreased B12 absorption despite adequate intake.
- Individual Genetic Variations – Genetic differences significantly impact vitamin utilisation. For instance, variants in the MTHFR gene (Methylenetetrahydrofolate reductase, an enzyme involved in folate processing) affect folate metabolism, whilst BCMO1 gene (Beta-carotene 15,15′-monooxygenase 1) variations influence how efficiently beta-carotene (plant-based vitamin A precursor) converts to vitamin A.
External factors like food processing methods also affect bioavailability. Heat treatment can destroy heat-sensitive vitamins like thiamin and vitamin C. Conversely, specific cooking methods may enhance the availability of some nutrients by breaking down cellular structures that would otherwise hinder absorption.
The timing of consumption plays a role as well. Some vitamins micronutrient compounds compete for absorption pathways, potentially reducing bioavailability when taken simultaneously in high doses. This explains why certain supplements are recommended at different times of day for optimal absorption.
Comprehensive Vitamins Micronutrient Reference Guide
Examining the full spectrum of vitamins micronutrient compounds requires looking at their key characteristics across multiple dimensions. The reference table below provides a detailed breakdown of essential information for all 13 vitamins.
Vitamins Micronutrient Reference Guide
µg = microgram | mg = milligram | IU = International Unit | RAE = Retinol Activity Equivalents (Vitamin A) | NE = Niacin Equivalents (Vitamin B3) | DFE = Dietary Folate Equivalents (Folate) | UL = Tolerable Upper Intake Level (maximum daily safe intake) | AI = Adequate Intake | NAD+/NADP+ = Nicotinamide Adenine Dinucleotide/Phosphate | FAD/FMN = Flavin Adenine Dinucleotide/Flavin Mononucleotide | GI = Gastrointestinal
Detailed analysis of 13 essential vitamins across 8 metrics, including daily requirements, primary functions, and deficiency symptoms. This comprehensive vitamins micronutrient reference outlines absorption factors and critical nutrient interactions for optimal health maintenance.
The table above is a central resource for vitamins micronutrient information, organised into eight essential categories that provide a complete picture of each vitamin’s profile.
The table categories provide essential information about each vitamin’s properties and requirements:
Daily Requirement
Refers to the recommended intake levels necessary for optimal health, expressed in appropriate units (micrograms, milligrams, or international units). These values differ by age, sex, and life stage, with pregnant and lactating women typically needing higher amounts of specific vitamins.
For instance, adult men need 900 μg RAE (Retinol Activity Equivalents, a measure of vitamin A activity) of vitamin A daily, whilst women require 700 μg RAE.
Primary Functions
This section highlights each vitamin’s primary physiological role in the body. Vitamin B12, for example, supports red blood cell formation, neurological function, and DNA synthesis. Vitamin D regulates calcium and phosphorus absorption, promoting bone health and immune function.
Deficiency Symptoms
Outlines the clinical and subclinical signs that may develop when intake falls below required levels. These manifestations range from mild (fatigue, irritability) to severe (night blindness for vitamin A deficiency or beriberi for thiamin deficiency).
Toxicity & Upper Limits
Details potential adverse effects from excessive intake and established safety thresholds. Fat-soluble vitamins pose greater toxicity concerns due to their storage in body tissues. For vitamin A, the upper limit is 3,000 μg RAE daily, with excess causing liver damage and birth defects.
Best Food Sources
Identifies the richest dietary sources for each vitamin, helping plan balanced meals that meet nutritional needs. Vitamin C, for instance, appears abundantly in citrus fruits, strawberries, bell peppers, and broccoli.
Bioavailability Factors
Describes elements that enhance or impair absorption and utilisation. For example, fat improves vitamin K absorption, while oxidation can affect vitamin E, which reduces its effectiveness.
Nutrient Interactions
Explains how vitamins influence or depend upon other nutrients. Vitamin C enhances iron absorption, whereas high retinol (vitamin A) intake may interfere with vitamin D function. Recognising these relationships helps prevent unintended consequences when supplementing.
This detailed guide to vitamins micronutrient components serves as reference and educational tool, enabling informed decisions about diet, supplementation, and overall nutritional strategy.
Deficiency and Toxicity: Finding the Balance
Finding the optimal balance of vitamins micronutrient intake represents a crucial health consideration. Insufficient and excessive consumption carry significant health implications, creating a “Goldilocks zone” (an optimal middle range that’s neither too much nor too little) for vitamin nutrition.
Deficiency Landscape
Vitamins micronutrient deficiencies remain surprisingly common worldwide, affecting populations across economic boundaries. More than 2 billion people globally suffer from micronutrient deficiencies, with the primary nutrients lacking being iron, iodine, zinc, and vitamins A and B.
Current estimates show that micronutrient deficiencies affect more than half of all children under age five globally, with most experiencing multiple deficiencies simultaneously. Even in affluent nations, subclinical deficiencies exist due to:
- Poor dietary choices favouring processed foods over nutrient-dense options
- Increased nutrient requirements during pregnancy, adolescence, and older age
- Restrictive diets that eliminate food groups
- Medication interactions that impair absorption
- Physiological changes affecting absorption capacity
The health impacts of insufficient vitamins micronutrient consumption manifest across body systems. Vitamin D insufficiency, for instance, correlates with reduced muscle strength, poorer physical performance, and higher fall risk in older adults. Inadequate B vitamin intake alters protein metabolism, potentially decreasing muscle mass and strength.
Toxicity Considerations
Whilst deficiencies receive considerable attention, excessive intake, mainly through supplementation, presents equally essential health concerns. The risk profile varies significantly between fat-soluble and water-soluble vitamins.
Fat-soluble vitamins (A, D, E, K) accumulate in body tissues, creating potential toxicity with prolonged high intake. Historical examples illustrate this risk:
| Vitamin | Toxicity Manifestations | Key Findings |
|---|---|---|
| Vitamin A | Liver damage, bone defects, birth defects | Upper limit set at 3,000 μg RAE; excess retinol during pregnancy linked to birth defects |
| Vitamin D | Hypercalcaemia, kidney stones | Upper limit established at 100 μg (4,000 IU); higher levels can disrupt calcium metabolism |
| Vitamin E | Increased bleeding risk | High doses (≥400 IU) associated with hemorrhagic stroke risk and all-cause mortality |
The scientific perspective on antioxidant supplementation has evolved significantly. Early observational studies suggesting high vitamin E intake might reduce heart disease led to widespread supplement use.
However, landmark trials subsequently showed beta-carotene supplements increased lung cancer rates in smokers, whilst high-dose vitamin E failed to prevent cardiovascular disease and may increase mortality risk.
Finding Equilibrium
Achieving balanced vitamins micronutrient intake requires personalised approaches based on individual needs. Factors requiring consideration include:
- Genetic variations affecting vitamin metabolism and requirements
- Life stage and physiological status (growth, pregnancy, ageing)
- Activity levels and metabolic demands
- Existing health conditions affecting absorption or utilisation
- Medication interactions with vitamin absorption or metabolism
The “food first” approach has gained substantial support in nutrition science. Studies increasingly demonstrate that whole foods provide vitamin matrices with synergistic benefits that isolated supplements cannot replicate. For example, the health effects of blueberries depend on the interaction of multiple compounds, including anthocyanins, flavonoids, phenolic acids, and proanthocyanins, not just isolated nutrients.
Laboratory assessment offers valuable insights for personalised vitamins micronutrient management. Beyond measuring direct vitamin levels, functional markers provide more explicit pictures of nutritional status. For instance, methylmalonic acid (a compound that increases when B12 is deficient) and holotranscobalamin (the active form of B12) offer a better assessment of B12 status than standard serum B12 tests alone.

Historical Evolution of Vitamins Micronutrient Knowledge
Knowledge about vitamins micronutrient compounds has undergone remarkable transformation over the past century, with particularly significant developments occurring in recent decades. This evolution reflects both scientific advancement and shifting public health priorities.
Early Understanding (Pre-1990s)
The early history of vitamins micronutrient research focused primarily on identifying these compounds and connecting them to deficiency diseases. By the mid-20th century, scientists had identified all 13 essential vitamins and established their basic functions. The field then shifted toward defining recommended intake levels and implementing public health measures to prevent overt deficiencies.
During this period, athletes reported performance benefits from vitamin supplementation as early as 1939, when cyclists in the Tour de France noted improvements after taking vitamin supplements. However, early scientific research did not consistently support these subjective reports.
Athletes continued using high-dose supplementation throughout the latter half of the 20th century. During the 1972 Olympic Games, athletes reported consuming large quantities of vitamins to enhance performance. This practice persisted despite mixed scientific evidence regarding benefits beyond deficiency prevention.
Transformative Discoveries (1990s-2010)
This era brought significant shifts in vitamins micronutrient understanding and public health approaches:
Folate Fortification (Late 1990s)
- In 1998, mandatory folic acid fortification of enriched grain products was implemented to prevent neural tube defects.
- This initiative led to a marked decline in spina bifida and anencephaly cases.
- Average folate intakes increased, making folate deficiency-related anaemia and birth defects less common.
Recognition of Choline (1998)
- The Institute of Medicine officially recognised choline as an essential nutrient.
- This acknowledgement came after studies showed humans develop fatty liver and muscle damage without sufficient choline.
- Choline was established as critical for foetal brain development and cognitive function.
Vitamin D RDA Increase (2010)
- The recommended daily allowance for vitamin D tripled from 200 IU to 600 IU for most age groups.
- The tolerable upper limit increased from 2,000 IU to 4,000 IU
- This adjustment reflected a consensus that previous recommendations were insufficient for optimal bone health
Antioxidant Perspective Shifts
- The ATBC (1994) and CARET (1996) trials unexpectedly showed beta-carotene supplements increased lung cancer rates in smokers.
- Extensive trials in the 2000s indicated that high-dose vitamin E not only failed to prevent cardiovascular disease but was associated with increased mortality.
- These findings dramatically reversed the “antioxidants for everyone” philosophy that had dominated earlier thinking.
Contemporary Understanding (2010-Present)
The current era of vitamins micronutrient knowledge has been characterised by more nuanced understandings and personalised approaches:
Expanded Vitamin D Roles
- Traditionally known for bone health, vitamin D has been intensively studied for broader roles in immune modulation, muscle function, and protection against diseases like colorectal cancer.
- Research during the COVID-19 pandemic spurred an additional investigation into vitamin D’s role in the immune response to respiratory infections.
- The scientific community now recognises vitamin D as a vitamin with wide-reaching importance beyond rickets.
Personalised Nutrition Emergence
Advances in nutrigenomics revealed how genetic variants affect vitamin utilisation:
- MTHFR gene mutations can impair folate metabolism
- BCMO1 variants affect beta-carotene conversion efficiency to vitamin A
- These findings suggest that “one size may not fit all” in vitamin nutrition
Food-First Philosophy Return
- Guidelines now emphasise obtaining nutrients through food rather than supplements.
- This shift followed disappointment in some supplementation trials and recognition that whole foods provide matrices (fibre, phytonutrients) that isolated vitamins lack.
- The dietary guidelines stress that nutritional needs should be met primarily from foods, not supplements.
Vitamins micronutrient knowledge continues to evolve as research methodologies advance and longer-term studies complete. Future directions may include more personalised vitamin recommendations based on genetic profiles, precise mechanisms of action, and interaction effects with the microbiome and other physiological systems.
Sources
- Abrams G.D., Feldman D., Safran M.R. Effects of Vitamin D on Skeletal Muscle and Athletic Performance. J. Am. Acad. Orthop. Surg. 2018;26:278–285.
- Bartali B, Semba RD, Frongillo EA, Varadhan R, Ricks MO, Blaum CS, Ferrucci L, Guralnik JM, Fried LP. Low micronutrient levels as a predictor of incident disability in older women. Arch Intern Med. 2006;166:2335–2340.
- Berger M.M., Shenkin A., Schweinlin A., Amrein K., Augsburger M., Biesalski H.K., Bischoff S.C., Casaer M.P., Gundogan K., Lepp H.L., et al. ESPEN micronutrient guideline. Clin. Nutr. 2022;41:1357–1424.
- Doseděl M., Jirkovský E., Macáková K., Krčmová L.K., Javorská L., Pourová J., Mercolini L., Remião F., Nováková L., Mladěnka P., et al. Vitamin C-Sources, Physiological Role, Kinetics, Deficiency, Use, Toxicity, and Determination. Nutrients. 2021;13:615.
- Houston D.K., Tooze J.A., Neiberg R.H., Hausman D.B., Johnson M.A., Cauley J.A., Bauer D.C., Cawthon P.M., Shea M.K., Schwartz G.G., et al. 25-hydroxyvitamin D status and change in physical performance and strength in older adults. Am. J. Epidemiol. 2012;176:1025–1034.
- Institute of Medicine (US) Committee to Review. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. National Academies Press (US); Washington, DC, USA: 1997.
- Kennedy D. B vitamins and the brain: Mechanisms, dose and efficacy—a review. Nutrients 2016;8(2):68.
- Lee G.Y., Han S.N. The Role of Vitamin E in Immunity. Nutrients. 2018;10:1614.
- Mayer J, Bullen B. Nutrition and athletic performance. Physiol Rev. 1906;40:369–97.
- Murdaca G., Tonacci A., Negrini S., Greco M., Borro M., Puppo F., Gangemi S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019;18:102350.
- Mustacich D.J., Bruno R.S., Traber M.G. Vitamin E. Vitam. Horm. 2007;76:1–21.
- National Institutes of Health (NIH), Office of Dietary Supplements (ODS). Folate Fact Sheet for Health Professionals.
- National Institutes of Health (NIH), Office of Dietary Supplements (ODS). Vitamin A and Carotenoids Fact Sheet for Health Professionals.
- National Institutes of Health (NIH), Office of Dietary Supplements (ODS). Vitamin B12 Fact Sheet for Health Professionals.
- National Institutes of Health (NIH), Office of Dietary Supplements (ODS). Vitamin E Fact Sheet for Health Professionals.
- Noriega-González D.C., Drobnic F., Caballero-García A., Roche E., Perez-Valdecantos D., Córdova A. Effect of Vitamin C on Tendinopathy Recovery: A Scoping Review. Nutrients. 2022;14:2663.
- Polegato B.F., Pereira A.G., Azevedo P.S., Costa N.A., Zornoff L.A.M., Paiva S.A.R., Minicucci M.F. Role of Thiamin in Health and Disease. Nutr. Clin. Pr. 2019;34:558–564.
- Powers S.K., Goldstein E., Schrager M., Ji L.L. Exercise Training and Skeletal Muscle Antioxidant Enzymes: An Update. Antioxidants. 2023;12:39.
- Quadros E.V. Folate and Other B Vitamins in Brain Health and Disease. Nutrients. 2023;15:2525.
- Rosanoff A., Dai Q., Shapses S.A. Essential nutrient Interactions: Does low or suboptimal magnesium status interact with vitamin D and/or calcium status? Nutr. 2016;7:25–43.
- Sămec D., Urlic B., Salopek-Sondi B. Kale (Brassica oleracea var. acephala) as a superfood: Review of the scientific evidence behind the statement. Crit. Rev. Food Sci. Nutr. 2019;59:2411–2422.
- Shahagadkar P., Shah H., Palani A., Munirathinam G. Berry derived constituents in suppressing viral infection: Potential avenues for viral pandemic management. Clin. Nutr. ESPEN. 2021;46:14–20.
- Shastak Y., Pelletier W. The Role of Vitamin A in Non-Ruminant Immunology. Front. Anim. Sci. 2023;4:1197802.
- Stevens GA, Bennett JE, Hennocq Q, Lu Y, De-Regil LM, Rogers L, et al. Trends and mortality effects of vitamin a deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. Lancet Global Health. (2015) 3–36.
- The Nutrition Source. Comment on the IOM Vitamin D and Calcium Recommendations.
- Tsugawa N., Shiraki M. Vitamin K Nutrition and Bone Health. Nutrients. 2020;12:1909.
- Uwitonze A.M., Razzaque M.S. Role of magnesium in vitamin D activation and function. J. Am. Osteopath. Assoc. 2018;118:181–189.
- Zeisel SH, da Costa KA. Choline: an essential nutrient for public health. Nutr Rev. 2009 Nov;67(11):615-23.

{kind=link}