

The market for CGM for non-diabetics has grown from a medical niche into a mainstream wellness habit. Once, doctors prescribed the continuous glucose monitor (CGM) almost only for people with diabetes. Now healthy, curious people buy them to study their own bodies. They want to track how food, sleep, and exercise affect their blood sugar.
This interest did not appear by accident. Healthcare has been shifting from one-size-fits-all care towards a personal, data-led model. That shift gave rise to biological feedback, in which your own bodily data is used to change behaviour. For over twenty years, that idea has grown alongside wearable technology.
People without diabetes now reach for these monitors for three main reasons. They hope to sharpen metabolic health, prevent disease, or improve sporting performance. Here, though, lies the first problem. We still know very little about whether this feedback truly improves long-term health.
The stakes behind the question are real, not imagined. Prediabetes, where blood sugar sits above normal but below diabetes, affects around 720 million people worldwide. Without action, 37 to 70 per cent of them develop diabetes within four years. Lifestyle change, however, can prevent more than half of those cases.
Most of us also spend our waking hours in the fed state rather than fasting. This matters because the rise in glucose after a meal carries its own risks. Postprandial spikes, meaning the rises after eating, raise cardiovascular risk even when fasting glucose looks normal. So the after-meal picture, which a monitor captures well, is worth understanding.
For people with diabetes, these sensors are proven and powerful tools. For healthy bodies, the science is far less settled. Some researchers describe consumer use of these devices as an evidence-free zone. Marketing, meanwhile, often frames a normal rise in glucose as a fault to be fixed.
The choice facing a healthy person is therefore not simple. A sensor can teach, yet it can also mislead, frighten, or empty a wallet. People may change their diet, fear ordinary spikes, or trust an app over proper screening. The promise of CGM for non-diabetics is real in places, but oversold in others.
What follows is a complete, honest reckoning with that promise. We begin with what the device measures, and the surprising amount it does not. We trace why interest has exploded, then weigh the evidence group by group. We look at how food, movement, sleep and stress bend your glucose line.
We count the true costs, including the quiet toll on peace of mind. Then we reach the only question that matters. Should the sensor go on your arm, or would your money and attention be better spent elsewhere?
What a CGM Measures and What It Does Not
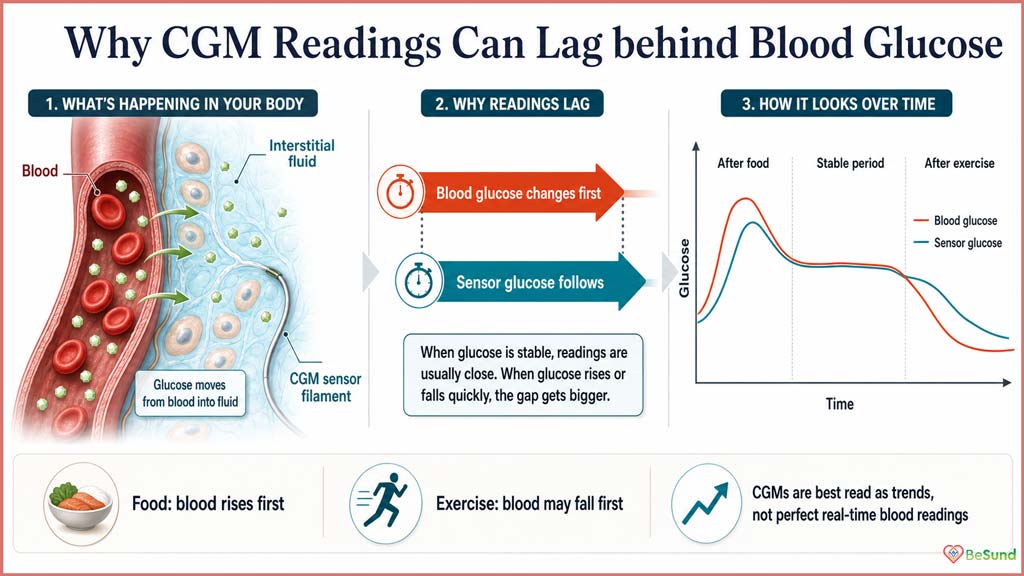
A continuous glucose monitor (CGM) is a small sensor worn on the upper arm or abdomen. A fine filament under the skin measures glucose in your interstitial fluid. That fluid surrounds your cells, sitting just below the skin surface. The sensor then sends readings to a phone or reader, often every few minutes.
Most sensors last up to two weeks, while some implanted versions read for months. Many also alert the user when glucose levels climb too high or drop too low. The technology first reached patients in 1999, by prescription, for insulin-dependent diabetes. Across two decades, the sensors became smaller, cheaper and far easier to wear.
For most of medical history, glucose could only be measured in a laboratory. Lab analysis remains the gold standard, accurate across a wide range of values. Home finger-prick meters followed, trading some accuracy for a single drop of blood. A continuous monitor goes further still, replacing single snapshots with a near-constant stream. The appeal of CGM for non-diabetics rests largely on that unbroken flow of data.
A monitor does not measure blood sugar directly, and that distinction matters greatly. Interstitial glucose closely tracks blood glucose, yet it always lags behind. When blood sugar changes quickly, the fluid catches up only after a delay. This lag widens during exercise, when glucose levels can shift fast.
The size of that delay also differs from person to person. Scar-like tissue forming around the sensor, called fibrotic encapsulation, is the main cause. Such differences help explain why accuracy varies from one body to another. For pinning down the exact response to a single food, a fingertip sample remains the criterion method.
Accuracy itself is summarised by a value called MARD, the mean absolute relative difference. Lower numbers indicate closer agreement with the true blood glucose level. Leading sensors meet international standards, yet differences from blood values must always be expected. Common substances can interfere, too, including paracetamol, which can distort some readings.
A monitor reveals trends, but it does not diagnose diabetes or prediabetes. Diagnosis still rests on standard blood tests, read within a clinical context. Doctors rely on fasting glucose, the oral glucose tolerance test, and HbA1c. HbA1c, or glycated haemoglobin, measures your average blood sugar over the past two to three months. It works by measuring how much glucose binds to haemoglobin, the oxygen-carrying protein in your red blood cells.
Those tests carry clear thresholds for prediabetes. A fasting glucose of 5.6 to 6.9 mmol/L signals impaired fasting glucose. An HbA1c of 5.7 to 6.4 per cent also falls in the prediabetes range. This limit matters for CGM for non-diabetics, where people test themselves without symptoms or medical guidance.
Yet each standard test captures only one moment and cannot be easily repeated. Here, continuous data adds something genuinely new. A single sensor worn for 10 to 15 days maps real-world glucose at home and at work. It can reveal patterns that a one-off test would miss completely. HbA1c, for instance, hides the short-term swings known as glycaemic variability.
Most apps turn a restless 24-hour signal into a handful of simple metrics. Each one describes a different feature of the same glucose line:
- Peaks: the high points your glucose reaches after food, stress or a poor night.
- Dips: the lower swings that follow, which can leave you hungry or shaky.
- Time in range: the share of the day spent inside a healthy glucose band.
- Variability: how much the line swings, captured best by the coefficient of variation.
- Baseline trend: the slow drift of your resting glucose across days and weeks.
These metrics have rough reference points in people without diabetes. Healthy adults spend about 96% of the day in range. They average around 99 mg/dL (5.5 mmol/L) over 24 hours. Time above 140 mg/dL stays uncommon, and may itself hint at future diabetes risk.
Even so, healthy glucose is not perfectly flat, and was never meant to be. People without diabetes still cross higher thresholds briefly during a normal day. In one study, normoglycaemic people reached impaired-tolerance levels several times daily. A small share even touched diabetic levels for short, harmless spells.
Researchers have sorted these patterns into glucotypes. People are grouped as having low, moderate, or severe glucose levels based on how much their glucose levels fluctuate. A severe glucotype does not equal disease, though it can flag hidden variability. A brief rise after a meal is therefore normal physiology, not a warning light.
Why CGM for Non-Diabetics Is Growing Now
A few years ago, wearing a continuous glucose monitor without diabetes seemed eccentric. That has changed fast. In several countries, you can now buy one over the counter, without a prescription. The global market mirrors this surge. Its value should climb from $5.2 billion in 2021 to $16.1 billion by 2030.
Uptake has risen sharply, even among people who medically do not need a sensor. In one large national survey, use increased from 0.4 per cent to 4.1 per cent between 2014 and 2020. Early adopters tended to be younger, employed, insured and on higher incomes. Prescriptions are also rising rapidly in routine care, especially in general practice.
The appeal of CGM for non-diabetics rests on a simple, seductive promise. You will finally see what your food does to you, in real time. That live feedback lets people adjust diet and activity on the spot. It speaks directly to common worries, about spikes, weight, insulin resistance and long-term risk.
Around this promise, an industry of apps and services has grown. Many translate a messy glucose signal into a tidy score for each meal. Artificial intelligence now further sharpens the picture. Some apps forecast glucose hours ahead and warn of a coming low.
The hardware itself is becoming gentler and less invasive. Newer designs use tiny microneedles that barely pierce the skin. Developers are even chasing needle-free glucose readings through a wristwatch. One prototype tracks blood glucose via radiofrequency, with no finger-prick required and no calibration.
These advances sound impressive, yet a caution belongs here. Most non-invasive tools cannot yet match the accuracy of established sensors. Early watch results came from controlled laboratories, not messy daily life. So tomorrow’s effortless gadget remains a work in progress, not a finished promise.
All of this has opened a curious gap in time. Demand for CGM for non-diabetics is racing ahead of the evidence behind it. Commercial pages often promise benefits faster than studies can support them. They can turn an uncertain, personal signal into a confident verdict on your lunch.
For now, most people pay for these sensors out of their own pockets. In future, they may be recommended by doctors and covered by insurance. Until then, buyers must meet the claims largely on their own, without a clear framework. That gap is exactly what an honest, evidence-led guide can fill.
![]()
The Evidence for CGM for Non-Diabetics
Evidence is not one solid block. It bends with the population you study. For people with diabetes, the ground is firm. As you move towards healthy bodies, it grows soft underfoot. The picture changes group by group.
In Diabetes: Strong and Proven
In diabetes, the benefit is clear and well measured. A review of 25 randomised trials, pooling data from 2,996 adults who used sensor feedback. On average, it lowered HbA1c by 0.28% and raised time in range by 7.4%. A reduction of more than 0.3% already counts as clinically meaningful.
That 7.4% gain clears the 5% threshold that many experts consider significant. Other reviews agree that monitoring reliably lowers HbA1c in type 2 diabetes. Real programmes show it too. In newly diagnosed type 2 diabetes, one study paired a sensor with a lower glycaemic-index diet. Within three months, HbA1c fell by 1% and weight by 7.2 kilograms.
One detail, however, deserves close attention. The same large review found no significant effect on weight or body mass index. So even in diabetes, the sensor sharpens control, yet does not melt away fat. That distinction will matter once we reach the weight-loss claims.
In Prediabetes and Higher Risk: Promising Signals
Move to prediabetes, and the case stays genuinely interesting. Here, a sensor can outperform standard blood tests at catching trouble. In one population, it found disordered glucose that fasting tests and HbA1c had missed. It can even separate normal from impaired glucose tolerance when HbA1c looks identical.
Glycaemic variability, the size of the daily swings, runs higher in prediabetes. It also tends to rise as the insulin-producing beta cells weaken. Using variability alone, one model sorted people by glucose health with 91% accuracy. Among overweight adolescents, those with prediabetes showed higher peaks and longer time above range.
Lifestyle programmes for high-risk people have used sensors with some success. A 12-week app-and-sensor programme increased time in range, reduced carbohydrate intake, and reduced weight. In prediabetes, low-carbohydrate coaching with a sensor lowered HbA1c and weight, with high satisfaction. Prediabetes is not harmless either. It already brings measurable damage to the smallest blood vessels.
In Athletes: Useful but Narrow
For sport, the evidence is real but specific. The clearest lesson is that steady fuel beats sky-high glucose. In endurance runners, a calm, well-supplied glucose level was associated with better performance than dramatic peaks. One marathon study even found the best running came with the flattest glucose curve.
The data can also map recovery after very hard training. After exhausting exercise, glucose patterns shift, then settle as the body recovers. Tracking that return may signal when an athlete is ready to train again. This is a precise, narrow use, not a reason for everyone to track food.
In Generally Healthy Adults: The Evidence Thins
Among healthy adults, honesty demands real caution. When we judge the evidence for CGM for non-diabetics, the gaps grow wide. Short use can lift awareness, and even ten days improved time in range for some. Sensors have also nudged inactive people towards more daily movement.
Awareness, though, is not the same as lasting health. Long-term outcomes and weight-loss claims stay largely unproven in healthy people. Many trials never even recorded diet, activity or time in range. So the mechanism behind any benefit often went unconfirmed.
The deeper problem concerns what variability actually predicts. In people without diabetes, it shows no clear tie to insulin sensitivity or blood pressure. It is not clearly linked to body fat, blood fats, or fatty liver either. Most studies are snapshots, so they cannot prove the swings cause later disease.
This is why established markers still matter most. HbA1c, fasting glucose, blood pressure, blood fats and fitness remain the validated yardsticks. A sensor adds texture around them, yet it does not replace them. The honest verdict on CGM for non-diabetics is therefore split by who you are.
Even so, a continuous glucose monitor can reveal hidden patterns worth knowing. Some apparently healthy people spend hours each day with glucose levels above normal. In one tracking study, 15% of healthy people reached diabetic-range spikes. Among those with prediabetes, that figure climbed to 36%.
Do the Swings Harm a Healthy Heart or Brain?
This is the question the marketing answers too confidently. Some evidence does suggest post-meal spikes carry a cost. In non-diabetic people, sharp rises in blood glucose can stress the lining of blood vessels. Swinging glucose appears even more damaging than a steady high level.
Larger studies point the same way, with caution. Higher post-meal glucose has tracked with narrowed heart arteries, even at normal tolerance. Over nearly 20 years, the highest post-meal group had 2.7 times the mortality rate. Bigger glucose swings have also been linked to vulnerable plaque in arteries.
The brain may feel it too. In one long-term study, greater glucose variability in young adulthood was associated with weaker memory in midlife. That held even below the threshold for diabetes.
Here, though, the honest brakes go on. Much of this evidence comes from people who already carry risk. Crucially, most of these findings are associations, not proof of cause. In metabolically healthy people, the swings have not clearly predicted these outcomes.
So the danger is real enough to respect, yet unproven as a target. No trial shows that flattening a healthy person’s spikes protects the heart. The link deserves attention, not the certainty a sales page sells.
Food, Exercise, Stress, and Blood Sugar Spikes
Blood sugar is restless by nature. It answers to far more than the food on your plate. The same meal can produce two different readings on two different days. This single fact should reshape how anyone reads their glucose data.
Why the Same Meal Moves Differently
Timing alone can transform a meal’s effect. Eat an identical breakfast and lunch, and lunch may spike you twice as high. Your body runs on a clock, with insulin sensitivity higher in the morning. Evening meals, therefore, tend to raise glucose levels and keep them elevated longer.
Sleep and stress leave their marks as well. A poor night worsens the next morning’s response to the very same food. Stress then adds its own push. Cortisol and adrenaline, the stress hormones, raise blood glucose without a single bite eaten.
The list of influences runs longer still. Illness, the menstrual cycle, hard training, and even sex all shift the response. Hormones and body clocks pull the same meal in different directions. So a single reading rarely tells a clean story for CGM for non-diabetics.
What Shapes the Curve on Your Plate
Food composition still matters most for the size of a spike. Carbohydrate drives the rise, while fibre, protein and fat soften it. In adults without diabetes, more fibre per meal led to a flatter response. Indeed, each gram of fat, fibre or protein independently blunts the rise. Several everyday choices reliably calm the curve, although the effect varies between people:
- Fibre: vegetables and whole grains slow the climb, and feed helpful gut bacteria.
- Protein: it digests slowly, steadying absorption and blunting the post-meal rise.
- Fat: a little added fat slows stomach emptying, lowering the peak for many.
- Order and form: whole foods and mixed meals tend to flatten the response.
- A short walk: moving soon after eating trims both the peak and the dip.
One caution about food rules belongs right here. The glycaemic index, which ranks foods by their effect on blood glucose, is only a rough guide. It cannot capture how a real, mixed meal behaves in a real body. Responses are also deeply personal. For some food pairs, the usual ranking reverses in nearly half of people.
Some foods, even so, spike almost everyone. A breakfast of cornflakes and milk pushed 80% of one group into the prediabetic range. A higher-fibre, higher-fat meal of bread and peanut butter caused gentler rises. Carbohydrate sensitivity is personal too, so the same bread barely moves another person.
Personalised Nutrition, the Gut, and What It Cannot Promise
This personal variation is exactly what the big subscription plans sell. Their pitch begins from something genuinely true. A computer model can even learn which foods spike you, then suggest better swaps. Used well, that tailored advice has improved post-meal glucose.
The plans promise more than steadier numbers, though. They reach for mood, energy, gut health and lasting wellness. There is a thread of evidence here. A high-glycaemic-load diet has worsened mood and raised fatigue in healthy people.
Much of the story traces back to the gut. The mix of bacteria there shapes how you handle a meal. Fibre feeds helpful microbes that make butyrate, a compound linked to steadier metabolism. Some bacteria align with gentler glucose responses; others with sharper ones.
Here, though, the confident claims meet harder evidence. Your genes explain only a small part of these responses. So tests based on DNA alone are unlikely to predict them well. Reviewers also warn that the personal-response claims often overstate the proof.
The gut-health promise is shakier still. Glucose tells you little about your blood fats, which move differently. So a glucose plan cannot stand in for whole metabolic health. No trial yet shows that chasing flatter glucose improves the gut itself. The science is real, but the marketing runs well past it.
Movement, the Strongest Lever
If food sets the scene, movement often steals it. A slow walk after eating lowers the glucose rise and the two-hour curve. Even breaking up long bouts of sitting helps. The benefit can appear without any change on the bathroom scales.
Timing decides much of the effect. Activity soon after a meal helps far more than the same effort hours later. A short walk after dinner can blunt that evening spike too. Both endurance and resistance training improve longer-term control, by different routes.
The effect of exercise also lingers, then fades. A single session can raise insulin sensitivity for the next 11 to 16 hours. Stop training for just ten days, however, and that gain slips away. So consistency, rather than intensity, tends to protect steady glucose over time.
Why a Flat Line Is Not a Virtue
Here lies the trap that catches anxious trackers. A higher rise does not brand a food bad, and a flat line does not crown a diet best. The familiar 140 and 180 thresholds were drawn for diabetes care. They were never meant as risk lines for healthy people.
Chasing the lowest possible line can even backfire. A steep spike is often followed by a sharp dip below baseline. That dip, not the peak, predicts hunger and later snacking. This is where CGM for non-diabetics can quietly distort healthy eating.
Active bodies need the opposite of a permanently flat line. Well-timed carbohydrate before exercise can lift performance, not harm it. For an athlete, available fuel sometimes matters more than a tidy graph. A glucose curve, in the end, is information, not a verdict on your character.

Risks, Costs, and Misleading Readings
A glucose number feels like hard truth. Often, it is softer than it looks. Before trusting the screen completely, it helps to know its weak points. There are more of them than the marketing admits.
When the Number Misleads
The sensor estimates glucose, so it can drift from your actual blood. In healthy adults, it tends to read on the high side. On average, it overstated glucose by about 0.9 mmol/L. It also showed each peak 5 to 12 minutes late.
The errors grow when you count time spent too high. The sensor overstated time above range by more than threefold. Even after calibration against real blood, it still roughly doubled it. So a healthy person can look far worse on screen than in life.
It can also rank foods wrongly, which matters for diet choices. In one test, the sensor branded a fruit smoothie high in sugar. Finger-prick blood showed the opposite, a low response. Across seven foods, the ranking flipped for five of them.
Part of the trouble is structural, not a simple fault. Interstitial fluid, the fluid bathing your cells, has no agreed reference standard, unlike a proper blood test. So no official accuracy chain exists for these readings. The precision shown on your phone is therefore partly an illusion. The bias also varies by person, so no single correction fixes it for all.
The Bill, and What It Could Buy Instead
The hidden cost of CGM for non-diabetics is rarely the sticker price alone. The full bill mounts quietly, and mostly from your own pocket. Before the subscription tab arrives, it helps to set the real costs side by side:
- The sensors: one sensor costs roughly $36 to $87 and lasts one to two weeks.
- The programmes: a short coaching course with sensors can cost several hundred dollars.
- The interpretation: someone must make sense of the flood of data, and that time is rarely free.
- The trade-off: the same money could buy better sleep, food and proven screening.
Cost also quietly decides who takes part. These tools drift towards wealthier users, widening an already unfair gap. High prices have left useful technology underused for years. So the people most at risk are often the least able to afford it.
The Skin, and the Smaller Print
The sensor clings to your skin for days, so reactions are fairly common. Trials report roughly one skin event per 8 weeks of wear. Most are mild, usually involving redness, itching, or slight hardening of the skin. Across studies, fewer than 2% of reactions were severe.
Even so, skin trouble is the top reason people stop using sensors. The cause is often an allergy to the adhesive glue. Real-world surveys suggest most long-term users experience some skin reaction. On the brighter side, most people find a sensor less painful than daily finger pricks.
The Mind: When Tracking Turns on You
Here lies the sharpest caution for CGM for non-diabetics. The biggest risk sits not in the skin, but in the head. Constant self-tracking can harm well-being and body image, especially among young people. A health tool can slowly become a source of anxiety.
The pattern is well documented with food and fitness apps. Many users report obsessive logging, guilt, and rigid rules around eating. Some skip meals once a number crosses a line they set for themselves. Others feel they must obey the app rather than their own body.
For some people, this tips into disordered eating. Among adults with eating disorders, most had used a calorie-tracking app. Nearly three-quarters felt the app had fed their illness. Doctors now often advise vulnerable patients to drop such trackers entirely.
A meal is not an exam to pass or fail. When every bite becomes a test, the simple pleasure of eating drains away. A glucose sensor can sharpen that pressure, turning normal food into a daily judgement. This risk deserves as much weight as any number on the screen.
Who Profits, and Who Holds Your Data
Money shapes the science more than most readers realise. In one review of behaviour-change trials, 44% declared ties to sensor makers. Among cost studies, 15 of 19 were funded by device companies. Such funding does not erase the findings, yet it colours them.
Your data carries value too, and it rarely stays private. Many health apps share information with outside companies. One review found most apps passing data to third parties, often without clear consent. Many label themselves wellness tools, which sidesteps stricter medical privacy rules. So your body’s story can travel further than you ever intended.

When CGM for Non-Diabetics May Be Useful, and When It May Not
Usefulness is not a property of the device. It depends entirely on the person wearing it. For one body, it teaches something real; for another, it sells noise as insight. The honest answer, then, sorts people into clear groups.
Start with those who carry real risk. A family history, a history of gestational diabetes, or warning symptoms each warrant a closer look. A sensor can catch early signs that standard tests sample only once. These include stubborn morning highs that often precede type 2 diabetes.
In prediabetes, the data can do something the usual tests cannot. It can sort people by glucose health, sometimes better than HbA1c. Variability itself may mark the slide from normal control towards diabetes. Some people with severe hidden patterns are missed entirely by standard tests. For them, an early warning means action while change is still easy.
Used alongside a doctor, that early picture has genuine worth. The clearest case for CGM for non-diabetics is a real question, not a vague worry. A short, guided trial can answer that question, then stop. This is monitoring with a purpose, rather than monitoring for its own sake.
Athletes have their own legitimate use, kept tightly focused. A sensor can test fuelling for a single event or a single hard session. That asks a precise, answerable question about performance. In rough conditions like high altitude, where finger-pricks read poorly, it can help too.
Now the weaker cases, which cover most healthy users. Many simply want one tidy score for their metabolism. No such score exists. There are no agreed-upon action thresholds, and no trial has proven that the swings harm healthy people.
A sensor will not hand you a weight-loss shortcut. Recall that even in diabetes, monitoring did not reduce weight on its own. Nor will it give reassurance with any real weight behind it. For precise food comparisons, a finger prick still beats the sensor.
Some hopeful uses simply outrun the evidence. In pregnancy, for example, the case for routine monitoring stays largely unproven. For most healthy people, the same holds true of daily glucose tracking. The promise of CGM for non-diabetics outpaces what the science can yet support.
If you still want to try one, a few principles keep it honest. They turn a vague experiment into a focused, time-limited test:
- Begin with a question: pick something specific, like your breakfast or your evening walk.
- Keep it brief: two to four weeks is usually enough to learn your patterns.
- Anchor it in proof: check anything worrying against fasting glucose, HbA1c, or your doctor.
- Guard your peace: if numbers start breeding fear or restriction, take the sensor off.
A continuous glucose monitor is a mirror, not a referee. It can show you something true, yet it cannot tell you who you are. For most healthy people, the oldest advice still wins. Sleep well, move often, eat with care, and see a doctor when something feels wrong.
A sensor may spark a little curiosity, and that is no bad thing. The trouble only begins when a passing number starts running your life. Worn with a clear question and a calm mind, it can teach. Worn out of fear, it mostly takes peace and money in return.
Sources
- Acciaroli G, Sparacino G, Hakaste L, Facchinetti A, Di Nunzio GM, Palombit A, Tuomi T, Gabriel R, Aranda J, Vega S, et al. Diabetes and Prediabetes Classification Using Glycemic Variability Indices From Continuous Glucose Monitoring Data. J Diabetes Sci Technol. 2018;12:105-113.
- Ajjan RA, Seidu S, Riveline JP. Perspective of continuous glucose monitoring-based interventions at the various stages of type 2 diabetes. Diabetes Ther. 2024;15(8):1657-1672.
- Akasaka T, Sueta D, Tabata N, et al. Effects of the mean amplitude of glycemic excursions and vascular endothelial dysfunction on cardiovascular events in nondiabetic patients with coronary artery disease. J Am Heart Assoc. 2017;6(5).
- Asarani NAM, Reynolds AN, Boucher SE, de Bock M, Wheeler BJ. Cutaneous Complications With Continuous or Flash Glucose Monitoring Use: Systematic Review of Trials and Observational Studies. J Diabetes Sci Technol. 2020;14(2):328-337.
- Asnicar F, Berry SE, Valdes AM, et al. Microbiome connections with host metabolism and habitual diet from 1,098 deeply phenotyped individuals. Nat Med. 2021;27(2):321-332.
- Bancks MP, Carnethon MR, Jacobs DR Jr, et al. Fasting glucose variability in young adulthood and cognitive function in middle age: the coronary artery risk development in young adults (CARDIA) study. Diabetes Care. 2018;41(12):2579-2585.
- Battelino T, Lalic N, Hussain S, et al. The use of continuous glucose monitoring in people living with obesity, intermediate hyperglycemia or type 2 diabetes. Diabetes Res Clin Pract. 2025;223:112111.
- Berry SE, Valdes AM, Drew DA, et al. Human postprandial responses to food and potential for precision nutrition. Nat Med. 2020;26(6):964-973.
- Blaak EE, Antoine J-M, Benton D, et al. Impact of postprandial glycaemia on health and prevention of disease. Obes Rev. 2012;13:923-984.
- Breymeyer KL, Lampe JW, McGregor BA, et al. Subjective mood and energy levels of healthy weight and overweight/obese healthy adults on high- and low-glycemic load experimental diets. Appetite. 2016;107:253-259.
- Ceriello A, Esposito K, Piconi L, et al. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes. 2008;57(5):1349-1354.
- Chai TY, Leathwick S, Agarwal MM, Sacks DB, Simmons D. Continuous glucose monitoring in gestational diabetes mellitus: hope or hype? Diabetes Res Clin Pract. 2025;227:112389.
- Cox DJ, Taylor AG, Moncrief M, et al. Continuous glucose monitoring in the self-management of type 2 diabetes: a paradigm shift. Diabetes Care. 2016;39(5):e71-e73.
- Dehghani Zahedani A, Shariat Torbaghan S, Rahili S, Karlin K, Scilley D, Thakkar R, Saberi M, Hashemi N, Perelman D, Aghaeepour N, et al. Improvement in Glucose Regulation Using a Digital Tracker and Continuous Glucose Monitoring in Healthy Adults and Those with Type 2 Diabetes. Diabetes Ther. 2021;12:1871-1886.
- Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393-403.
- Didyuk O, Econom N, Guardia A, Livingston K, Klueh U. Continuous Glucose Monitoring Devices: Past, Present, and Future Focus on the History and Evolution of Technological Innovation. J Diabetes Sci Technol. 2021;15(3):676-683.
- Echouffo-Tcheugui JB, Perreault L, Ji L, Dagogo-Jack S. Diagnosis and management of prediabetes: a review. JAMA. 2023;329(14):1206-1216.
- Ehrhardt N, Al Zaghal E. Behavior Modification in Prediabetes and Diabetes: Potential Use of Real-Time Continuous Glucose Monitoring. J Diabetes Sci Technol. 2019;13(2):271-275.
- El Sayed NA, Aleppo G, Aroda VR, et al. Classification and diagnosis of diabetes: standards of Care in Diabetes 2023. Diabetes Care. 2023;46(Suppl 1):S19-S40.
- ElSayed NA, Aleppo G, Bannuru RR. Diagnosis and classification of diabetes: standards of care in Diabetes 2024. Diabetes Care. 2024;47(Suppl 1):S20-S42.
- Fogh-Andersen N, Altura BM, Altura BT, Siggaard-Andersen O. Composition of Interstitial Fluid. Clin Chem. 1995;41:1522-1525.
- Guess N. The growing use of continuous glucose monitors in people without diabetes: an evidence-free zone. Pract Diabetes. 2023;40(5):19a-22a.
- Hall H, Perelman D, Breschi A, Limcaoco P, Kellogg R, McLaughlin T, Snyder M. Glucotypes Reveal New Patterns of Glucose Dysregulation. PLoS Biol. 2018;16:e2005143.
- Heinemann L, Schoemaker M, Schmelzeisen-Redecker G, et al. Benefits and limitations of MARD as a performance parameter for continuous glucose monitoring in the interstitial space. J Diabetes Sci Technol. 2020;14(1):135-150.
- Herrero P, Andorra M, Babion N, et al. Enhancing the Capabilities of Continuous Glucose Monitoring With a Predictive App. J Diabetes Sci Technol. 2024;18(5):1014-1026.
- Hirsch IB, Tirosh A, Navon A. Noninvasive Real-Time Glucose Monitoring Is in the Near Future. Diabetes Technol Ther. 2024;26(9):661-666.
- Hjort A, Iggman D, Rosqvist F. Glycemic variability assessed using continuous glucose monitoring in individuals without diabetes and associations with cardiometabolic risk markers: A systematic review and meta-analysis. Clin Nutr. 2024;43(4):915-925.
- Honary M, Bell BT, Clinch S, Wild SE, McNaney R. Understanding the Role of Healthy Eating and Fitness Mobile Apps in the Formation of Maladaptive Eating and Exercise Behaviors in Young People. JMIR Mhealth Uhealth. 2019;7(6):e14239.
- Huckvale K, Torous J, Larsen ME. Assessment of the Data Sharing and Privacy Practices of Smartphone Apps for Depression and Smoking Cessation. JAMA Netw Open. 2019;2(4):e192542.
- Hutchins KM, Betts JA, Thompson D, Hengist A, Gonzalez JT. Continuous glucose monitor overestimates glycemia, with the magnitude of bias varying by postprandial test and individual: a randomised crossover trial. Am J Clin Nutr. 2025;121(5):1025-1034.
- Ishihara K, Uchiyama N, Kizaki S, Mori E, Nonaka T, Oneda H. Application of Continuous Glucose Monitoring for Assessment of Individual Carbohydrate Requirement during Ultramarathon Race. Nutrients. 2020;12:1121.
- Joseph JI. Review of the Long-Term Implantable Senseonics Continuous Glucose Monitoring System and Other Continuous Glucose Monitoring Systems. J Diabetes Sci Technol. 2021;15:167-173.
- Jospe MR, Richardson KM, Saleh AA, et al. Leveraging continuous glucose monitoring as a catalyst for behaviour change: a scoping review. Int J Behav Nutr Phys Act. 2024;21(1):74.
- Klonoff DC, Nguyen KT, Xu NY, et al. Use of continuous glucose monitors by people without diabetes: an idea whose time has come? J Diabetes Sci Technol. 2022;0(0):1-12.
- Levinson CA, Fewell L, Brosof LC. My Fitness Pal calorie tracker usage in the eating disorders. Eat Behav. 2017;27:14-16.
- Lunde MS, Hjellset VT, Hostmark AT. Slow post meal walking reduces the blood glucose response: an exploratory study in female Pakistani immigrants. J Immigr Minor Health. 2012;14(5):816-822.
- Nathan DM, Davidson MB, DeFronzo RA, et al. Impaired Fasting Glucose and Impaired Glucose Tolerance. Diabetes Care. 2007;30(3):753-759.
- Polaris Market Research. Continuous Glucose Monitoring Device Market Size, Analysis Report, 2025-2034. 2024.
- Richardson KM, Jospe MR, Bohlen LC, Crawshaw J, Saleh AA, Schembre SM. The efficacy of using continuous glucose monitoring as a behaviour change tool in populations with and without diabetes: a systematic review and meta-analysis of randomised controlled trials. Int J Behav Nutr Phys Act. 2024;21(1):145.
- Rodriguez-Segade S, Rodriguez J, Camina F, et al. Continuous glucose monitoring is more sensitive than HbA1c and fasting glucose in detecting dysglycaemia in a Spanish population without diabetes. Diabetes Res Clin Pract. 2018;142:100-109.
- Rohleder N. Stress and Inflammation: The Need to Address the Gap in the Transition between Acute and Chronic Stress Effects. Psychoneuroendocrinology. 2019;105:164-171.
- Sasso FC, Carbonara O, Nasti R, et al. Glucose metabolism and coronary heart disease in patients with normal glucose tolerance. JAMA. 2004;291(15):1857-1863.
- Senn S. Mastering variation: variance components and personalised medicine. Stat Med. 2016;35(7):966-977.
- Shah VN, DuBose SN, Li Z, Beck RW, Peters AL, Weinstock RS, Kruger D, Tansey M, Sparling D, Woerner S, et al. Continuous Glucose Monitoring Profiles in Healthy Nondiabetic Participants: A Multicenter Prospective Study. J Clin Endocrinol Metab. 2019;104:4356-4364.
- Sherrill CH, Lee S. Prevalence, characteristics, and health-related quality of life of continuous glucose monitoring use according to the Behavioral Risk Factor Surveillance System 2014-2020. J Manag Care Spec Pharm. 2023;29(5):541-549.
- Tsereteli N, Vallat R, Fernandez-Tajes J, et al. Impact of insufficient sleep on dysregulated blood glucose control under standardised meal conditions. Diabetologia. 2022;65:356-365.
- S. Food and Drug Administration. FDA Clears First Over-the-Counter Continuous Glucose Monitor. Published March 6, 2024.
- Vaccaro O, Ruth KJ, Stamler J. Relationship of postload plasma glucose to mortality with 19-yr follow-up. Comparison of one versus two plasma glucose measurements in the Chicago Peoples Gas Company study. Diabetes Care. 1992;15(10):1328-1334.
- Wyatt P, Berry SE, Finlayson G, et al. Postprandial glycaemic dips predict appetite and energy intake in healthy individuals. Nat Metab. 2021;3:523-529.
- Zeevi D, Korem T, Zmora N, et al. Personalised Nutrition by Prediction of Glycemic Responses. Cell. 2015;163(5):1079-1094.

{kind=link}