

The boom in red light therapy has slipped into bathrooms, gyms, clinics and bedrooms. It carries the quiet confidence of something that has gone mainstream. Masks. Panels. Mats. Beds the size of a small car. Wands that look like a remote control from the future.
In research papers, the category goes by a different name. Photobiomodulation, usually shortened to PBM, meaning the use of low-level red and near-infrared light to act on living cells.
Most people will never use that word. Most people just call it a red light. And it has reached the moment where the question shifts. It is no longer “have you heard of it?”, but “should I buy one?”
Here is the honest scene. The biology is real. The strongest wins, in skin care and certain medical settings, are real. And the marketing, in places, has galloped well ahead of what has actually been shown in people.
Most writing on this topic takes sides. Either it lands as a miracle, or it lands as nonsense. Both pictures fail to show the person actually trying to decide.
Something quietly astonishing happens when red light meets a living cell. A photon is a tiny packet of light. It slips through the skin and is caught by an enzyme tucked inside a mitochondrion. A mitochondrion is the small structure inside cells that makes energy. Afterwards, the cell behaves differently. Energy production lifts. Inflammation calms. Repair pathways wake up. That is not folklore. That is the mechanism.
Yet two devices that both call themselves red light therapy can deliver wildly different exposures to your skin. Same colour. Same name on the box. Different result entirely. The dose is the whole game, and it’s rarely on the label.
So the real question is not “does it work”. The real question is sharper. For what purpose? At what dose? Using what device? Compared with what alternative? Hold that question in your hand.
This post is built to answer it. Plain English, with the science kept visible only where it earns its place. Some of what you find will surprise you. Some will sober you. The aim is simple. By the end, you should not be guessing.
What Is Red Light Therapy, and Why Is It Everywhere?
A short biology of how the field got its name is worth knowing. Red light therapy is the consumer phrase. The lab name is photobiomodulation, sometimes still called low-level laser or low-level light therapy. The shift to “photobiomodulation” happened for a reason. The same biological response could be triggered by a laser, a simple LED, or other non-coherent (non-laser) light sources. The word grew up to fit the science.
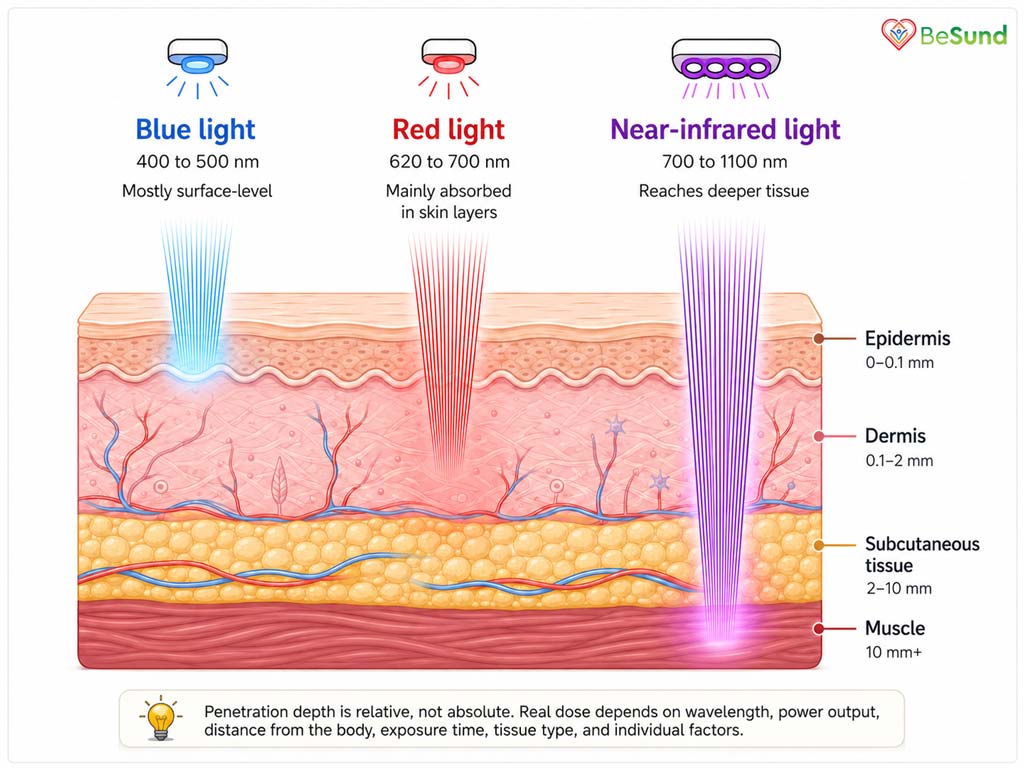
Two ingredients give you the colours that matter here. Visible red light, which is the deep red your eye can see. And near-infrared light, which sits just past where your eye stops. They behave differently in tissue. Red light is suited to surface targets such as the dermis (the layer of skin below the surface). Near-infrared reaches further, towards muscle, joint and deeper structures.
The therapy did not arrive from a marketing department. It started by accident in the late 1960s. A Hungarian researcher found that low-power laser exposure accelerated hair regrowth in shaved mice. The same kind of light helped stubborn human ulcers close. From those small, slightly strange beginnings, the field grew. It moved through dentistry, dermatology and physiotherapy, before quietly walking into the high street.
Why is it suddenly on every shelf?
Three things tipped it over. LEDs got cheap. They got safe enough to put in a home product without needing a trained operator, unlike early lasers. And the broader public mood turned firmly against anything that felt invasive, slow to recover from, or chemically heavy. A device that just glows at your face for ten minutes. No needles. No downtime. It fits that mood like a key into a lock.
The market answered. Masks. Panels you stand in front of. Mats you lie on. Wraps for joints. Beds you climb into at a wellness suite. Helmets are aimed at the scalp. Wands for the face. The same coloured light, dressed in very different clothes.
What red light is not
Worth saying clearly, because the confusion is everywhere. Red light therapy is not a tanning bed. Tanning beds use ultraviolet light, a higher-energy invisible light with well-known risks to the skin. Red and near-infrared sit at the gentler, longer-wavelength end of the spectrum. They are described as non-thermal. That means they should not heat or burn tissue when used correctly.
It is also not an infrared sauna. Saunas work by heat. Their benefits, where they exist, come from warming the body, not from light interacting with cells.
It is also not photodynamic therapy. That treatment uses light to switch on a separately delivered drug, to deliberately damage abnormal cells. The two are sometimes mixed up in marketing copy. They are different jobs done by different physicists.
How Red Light Therapy Is Supposed to Work
There is a quiet drama happening, and most people who buy a red light therapy mask never hear about it. It involves a single particle of light, a copper-and-iron enzyme, and a power station inside the cell.
Start with the enzyme. Its name is cytochrome c oxidase. It sits at the end of the breathing line inside a mitochondrion. A mitochondrion is the cell’s tiny power plant. Its job is to help turn the food you eat into the energy your body uses. When red or near-infrared light hits this enzyme, something interesting happens. The light is absorbed. The enzyme’s behaviour changes.
Often, a small molecule called nitric oxide has been clinging to the enzyme and slowing it down. The light dislodges it. The enzyme breathes more freely. Energy production lifts. The freed nitric oxide drifts into the surrounding tissue. It helps dilate small blood vessels, improving blood flow.
That is the headline. A photon is caught. An enzyme is freed. The cell finds a little more energy and a little better blood supply.
The next part is the part most marketing copy quietly skips. The cell does not just make more energy. It also receives a brief signal. A small puff of reactive oxygen species (molecules normally cast as villains) acts here as a messenger, not a weapon. That message reaches the nucleus and activates certain genes. Genes for repair. Genes that calm inflammation. Genes that build proteins involved in healing. Inflammatory chemicals such as TNF-α and IL-6 (proteins your body releases when something is wrong) can drop. Repair-friendly cells can be recruited.
It is a very polite kind of biology. Nothing is cut. Nothing is burned. The light simply nudges, and the cell responds.
But this is also where the field stops being romantic.
If too little light reaches the cell, nothing happens. If too much arrives, the cell ignores it, or worse, switches off the very response you wanted to encourage. The shape of this response has a name. The biphasic dose response. Low to moderate doses help. Higher doses help less, then stop helping, then begin to hurt. There is no straight line between more light and greater benefit. There is a sweet spot, and it is narrower than the marketing suggests.
The sweet spot of red light therapy also depends on what you are trying to reach. Surface skin. Joint tissue. Muscle a few centimetres down. The wavelength that suits one is wrong for another. The dose that suits one tissue does nothing for another. The cell with many mitochondria responds to less light. The cell with few may need more, or may not respond at all.
This is the part to carry forward. The mechanism is real and rather beautiful. The dose is everything. The colour on the box provides very little information. What matters is whether the light reaching your cell is the dose your cell can use.
What the Evidence Actually Shows
The evidence is messy in places, and unusually strong in others. The honest map looks like this. There are areas where red light therapy has earned its credibility through proper trials. There are areas where the data is encouraging but unfinished. And there are areas where the marketing has run into territory that science has not.
What follows is the first of those three groups. The places where the evidence has done its work.
Skin: lines, collagen, and the look of age
Skin is where most consumer interest lives, and it is also where the dermatology trials have been most active. A controlled trial of repeated red and near-infrared light treatment found measurable changes. Fine lines softened. Wrinkles reduced. Skin roughness eased. Collagen density in the dermis (the layer below the surface) lifted. Patient satisfaction was high. The effect was not dramatic. It was real.
A separate trial focused on the area around the eyes. It reported a roughly 30% reduction in wrinkle volume around the eye after a course of treatment. Modest. Repeatable. Measurable. That is the honest tone for skin.
Acne
Acne sits in the same encouraging-but-not-magic camp. A double-blind trial tested a home-use blue-red LED device in mild-to-moderate acne. It reported a roughly 77% reduction in inflammatory lesions over the course of treatment. Skin samples showed less inflammatory infiltrate and smaller sebaceous glands. Inflammatory acne tends to respond better than blackheads and whiteheads, which sit deeper and behave differently.
This is one of the more believable consumer-facing wins. It holds when the device parameters and the protocol resemble what was actually tested.
Radiation dermatitis and oral mucositis
Now, the strongest medical signal in the whole field. People undergoing radiotherapy for head and neck cancer often develop painful skin and mouth-lining damage that can interrupt their treatment. A multicentre placebo-controlled trial tested dual-wavelength photobiomodulation in this group.
It reduced moderate-to-severe radiation dermatitis by 49% by the end of treatment. A separate clinical programme used LED light to treat radiotherapy-related mucositis and dermatitis. It recorded no device-related adverse events across more than 1,300 exposures. Most existing lesions improved or stabilised.
If you take only one thing from this section, take this. The strongest evidence lies in oncology supportive care. Quietly. Without the marketing.
After surgery
After third molar surgery, an infrared diode laser cut pain and swelling at 24 and 48 hours. It outperformed sham treatment in a randomised, double-blind trial. After eyelid surgery, an LED protocol reduced swelling, pain and anxiety in a trial of 145 patients. No side effects were reported. The signal here is consistent. The body is already in repair mode after surgery, and the light appears to nudge it along.
Pain in the neck and joints
A pooled review of randomised trials on neck pain examined low-level laser therapy. Acute pain dropped straight after treatment. Chronic pain stayed lower for up to 22 weeks afterwards. In knee osteoarthritis, pooled data from more than a thousand participants told a similar story. Pain relief versus placebo at the end of treatment and through 1 to 12 weeks of follow-up. The benefit was clearer when recommended doses were used.
The pattern keeps repeating. Where the dose is right, and the target is inflammatory or repair-related, the relief is real and measurable.
Plantar fasciitis and tendinopathy
The heel-pain story is one of the most useful for everyday readers. Pooled data from randomised trials looked at lower-extremity tendinopathy and plantar fasciitis. Plantar fasciitis is the painful inflammation of the band along the bottom of the foot.
Low-level laser therapy cut pain straight after treatment by about 13 mm on a 100 mm scale. At 4 to 12 weeks, pain remained about 12.5 mm lower. Doses that matched recommended guidelines performed better than those that did not.
When the laser was added to exercise, stretching, and insoles, pain decreased further than with standard care alone. No adverse events were reported. The pain reductions for plantar fasciitis sat above the level usually considered clinically meaningful, not just statistically interesting.
Fibromyalgia, with one important condition
Fibromyalgia is a chronic, widespread pain condition. A trial of 160 women tested red light therapy against exercise, and against the two together. Light alone reduced pain meaningfully. Exercise alone reduced pain meaningfully.
The combination of light therapy plus exercise produced the largest drop in pain and tender points. The honest reading is that exercise remains the foundation. The light appears to add to it, not replace it.
Hair
The most commercially relevant hair evidence came from a randomised, sham-controlled trial of a laser comb. It involved 110 men with male-pattern hair loss. Hair growth improved significantly compared with the sham device.
The result was strong enough to secure regulatory clearance for efficacy. Later work in caps, helmets and handheld units has continued to report gains in hair density. This applies to androgenetic alopecia, the medical name for pattern hair loss.
Eyes and brain: small but interesting
A multicentre trial looked at the dry form of age-related macular degeneration. A multiwavelength protocol improved visual function over nine months. It also reduced the build-up of small retinal deposits called drusen. A separate randomised trial used near-infrared light through the scalp in adults over 50. Participants had mild cognitive impairment, an early decline in memory and thinking. Cognition improved. A brain-supporting protein called BDNF rose. Benefits persisted three months later.
These are small, careful trials. They are early, but they are nothing.
Across this whole map, two things stand out. The strongest wins are local, targeted, and used at the right dose. The weakest are the broad ones. That is the line to hold as we move on to the next group below.

Where Red Light Therapy Claims Start to Outrun the Science
Now the harder part. Some of the loudest claims for red light therapy sit a long way from the data. Not because the data is bad. Because the claim has stretched well past it.
Fat loss and body contouring
This one is everywhere, and the careful answer is uncomfortable. A 2025 pooled analysis of studies on light applied to the abdomen looked at the markers people actually care about. Body weight did not significantly change. Body mass index did not. Fat mass did not. Lean mass did not.
The signals that did appear were narrower. Waist circumference shifted. Hip circumference shifted. Insulin and triglycerides moved a little.
Read that again, because it matters. The waistline measurement can move without weight changing. Some inches without pounds is a real but modest effect. It is not the dramatic fat-loss story that some advertising suggests.
Sleep
The best research linking light therapy to sleep is in animals. It looks at how light at night may help the brain clear waste during sleep. That is genuinely interesting. It is also not the bedside mask. It involves nocturnal protocols aimed at brain-clearance pathways, in mice, in laboratories. Translating that to a wellness panel beside your bed is a leap the data has not made.
Mood
There is a real, careful line of work using transcranial near-infrared light for depression. Some early protocols showed promise. But a multicentre, randomised, sham-controlled trial of very-low-level transcranial light in major depressive disorder found no improvement compared with sham.
The likely reason is dose. Below a threshold, nothing happens. The protocols that have shown promise used specific wavelengths, irradiance levels, scalp-targeted geometry and treatment durations. A general consumer panel is not those protocols.
Sports performance
This is where the gap between belief and data is often largest. In well-trained cyclists, red light at 4.6 J/cm² before a Wingate test (a 30-second, all-out cycling sprint against high resistance) did not improve mean power, peak power, fatigue index or time to peak power.
In a six-week sprint and squat training programme in trained men, adding active light therapy did not produce any extra benefit over placebo or simple passive recovery. The training itself worked. The light added nothing on top.
The honest pattern looks like this. Red light therapy seems to do most for tissues under stress, in disease or in repair. It struggles to add much to a young, well-trained, well-recovering body that is already adapting nicely on its own.
Low back pain
Despite the broader pain wins covered earlier, low back pain has not shown a similar pattern. A randomised, placebo-controlled trial in chronic non-specific low back pain found that photobiomodulation was no better than placebo.
A systematic review reached a similar conclusion. It did not generally reduce pain in this group. The reasons may include dose, depth, or the unusual complexity of low back pain itself. The honest answer is that the evidence is not yet there.
Testosterone and “longevity”
These claims are loud online. The body of careful research underpinning this article does not directly speak to them. Where the data is silent, the right thing to do is to say so, and not to invent confidence on the reader’s behalf.
The broader trap
The trap most consumer claims fall into is borrowing. A clinical study used a calibrated, single-wavelength laser at a known dose under defined conditions, following a defined protocol. A consumer device emits red light. The two are described in the same breath, and the second inherits the first’s credibility. That borrowing is where most overreach comes from. It is not always dishonest. It is just sloppy, and the reader pays for it.
Why At-Home Devices Are Not the Same as Clinical Treatments
Two devices labelled as red light therapy can have very different effects on your body. That is not a manufacturing quirk. It is the heart of the field.
A clinical device is built around the dose. The wavelength is precise. The power output is calibrated. The treatment area is defined. The session length is set. The distance from the skin is set. The operator is trained to keep it that way. A home device is built around being usable while you watch television. Different design brief, different result.
Most of the research that built credibility for the field used lasers. That is not the type of LED found in most consumer products. LEDs are not inferior in principle. They simply deliver light differently.
A result obtained with one device cannot be quietly assumed for another. A sober review of home-based dermatology devices put it cleanly. Home use improves access and adherence. Neither of those proves the device delivers a clinically effective dose.
Then there is the gap between what a label says and what a body receives.
The numbers that actually matter
Wattage on a box is almost meaningless on its own. What matters is irradiance, the amount of light energy hitting each square centimetre of skin. Then fluence, the total dose delivered over time.
Then beam profile, because a laser beam concentrates power at the centre and tails off at the edge. Then distance, because power falls off quickly as you move away. Then, pulse mode, treatment area, contact versus non-contact, and how reflective your skin is at that moment.
A device can have impressive marketing wattage and still under-deliver to your tissue. Another can have humble specs and deliver something useful, if everything else is right. Consumers cannot judge any of this without the parameters being printed clearly on the box. Most are not.
The brain is the special case
Devices marketed at the head deserve particular caution. The human skull is not a friendly surface for light. Measurements taken through human cadaver heads tell the story. 830 nm light transmission through the temporal area was 0.9%. It was 2.1% through the frontal area, and 11.7% at the back of the head. Even the most generous of those numbers means most of the light never reaches the brain. By comparison, the mouse skull lets 40% of similar light through, and the rat lets 21%.
Most published animal “brain effects” of red light therapy were measured in skulls that the light could actually penetrate. Human anatomy does not extend that courtesy.
The takeaway for the buyer is not to give up on light through the head. It is to be sceptical of any claim that ignores the skull. Be sceptical of any claim that does not openly account for the dose at the actual target. Brain-targeted clinical research uses specific protocols, sometimes via intranasal routes, often across multiple sites, and carefully calibrated parameters. A wellness helmet borrowing that credibility without those parameters is asking the buyer for trust that science has not given.
A home device can still earn its keep, for the right job, in the right way. The trick is to know which job, and to check that the device can plausibly do it.

Skin, Pain, Recovery, and Wellness: What Looks Most Plausible?
A useful way to think about red light therapy is as a supportive tool, not a standalone cure. The places where it earns its keep tend to share a few things in common. The target is local. The tissue is under some kind of stress, undergoing repair, or showing low-grade inflammation. The dose is tailored to the condition being treated. The expectations are sensible.
For your skin
Skin is the most accessible and one of the most plausible uses. The light reaches the dermis without difficulty, and the cells that build collagen and elastin appear to respond. A randomised trial focused light on the area around the eye. It found roughly a 30% reduction in wrinkle volume after a course of treatment.
The effect is moderate and cumulative. It is the look of slightly fresher, slightly better-lit skin, not a different face.
For acne, the more inflammatory the lesion, the more responsive it tends to be. For wound and skin healing, an experimental red LED protocol calmed key inflammatory chemicals. It lowered IL-1β, IL-10 and TNF-α, and reduced oxidative stress in healing skin. The biology behind a “fresher complexion” is real enough when the device is appropriate.
For pain
Pain is one of the strongest non-skin areas. Neck pain. Knee osteoarthritis. Plantar fasciitis. Chronic joint problems. Where the dose is appropriate and the target is inflammatory, the relief is repeatable. The most useful framing here is supportive. Red light therapy appears to complement good physiotherapy, exercise, stretching, and basic care. It rarely replaces them.
For active people with achy joints or stubborn heel pain, that is actually the more honest sales pitch. Not a cure. An add-on that, used at the right dose, can take the edge off. It can help the more important interventions do their work.
For after surgery and after injury
The body in repair mode is unusually responsive. After eyelid surgery, an LED protocol reduced swelling, pain and anxiety. In a trial of 145 patients, no side effects were reported. The body had a job to do. The light appears to have helped it do that job slightly faster and slightly more comfortably. This is one of the more useful, under-discussed applications.
For recovery in active people
Here, the picture is more mixed than the marketing would suggest. There is a genuine mechanism. Light exposure raises the activity of the cell’s energy machinery. Mitochondrial output peaks around three to six hours after treatment.
There are positive trials. A double-blind crossover study tested high-level rugby players. A light protocol improved field-test performance and sped up short-term recovery.
But there are also null trials. Well-trained cyclists and trained men who completed a sprint-and-squat programme saw no additional benefit. The pattern that emerges is not “light therapy works for recovery” or “light therapy does not work for recovery”.
It is more nuanced. The benefit appears to be largest after exercise that genuinely damaged or stressed the muscle. It tends to disappear when the body has already adapted to the load. Timing matters too. Pre-exercise, post-exercise, with cold therapy, without it, all change the result.
For hair
Hair regrowth has an unusually credible mechanism, supported by its trial evidence. Light appears to push resting hair follicles into the active growing phase and may prolong that growing phase. It also widens the blood vessels around the follicle by releasing nitric oxide. And it calms local inflammation that disrupts follicle function. This is one of the few wellness uses where the consumer device evidence and the biology line up reasonably well.
For everything else
The honest reading is that the strongest, most defensible uses are local and targeted. Skin. Selected pain. Hair. Post-surgical and post-injury repair. Inflammatory tissues. Where it is sold as a broad boost to vitality, energy, immunity or wellness, the data is thinner. And the device the buyer is looking at is rarely the device that produced what data does exist.
That last point will not stop mattering. A finding belongs to a specific device, a specific dose and a specific tissue. It does not transfer just because the colour matches.
Safety, Side Effects, and Who Should Be Careful
For most people, used sensibly, red light therapy is a low-risk thing to try. The honest summary in the dermatology literature is reassuring. There is no evidence of DNA damage from red or near-infrared light, even at high doses. Side effects, when they appear, tend to be mild and short-lived. That is a reassuring starting position. It is not, however, a blanket licence to ignore the rest of this section.
What people most commonly notice
Mild warmth. A short-lived flush of redness on the skin. Occasionally, a mild headache, dry mouth, sleep disturbance, fatigue, or transient irritability after sessions aimed at the head. These tend to resolve within a day. They are the kind of thing a sensible person notices, adjusts for, and moves on from.
Where the dose itself becomes the safety story
This is the part to take seriously. Two randomised safety trials of red LED light at 633 nm found something worth noting. At 320 J/cm² and above, prolonged redness appeared in some lighter-skinned participants. At 480 J/cm² and above, blistering occurred across skin types. That is a useful reminder. Red light is gentle at sensible doses. It stops being gentle if the dose climbs.
The eye is its own story. A safety analysis examined red-light devices used to treat childhood myopia. Some of these devices, used as instructed, approached or exceeded the safe exposure limit for the retina.
A published case report described retinal damage in a 12-year-old. It followed five months of repeated exposure to a red-light laser device. The wider lesson is simple. Anything aimed at the eye, or capable of being aimed at the eye, deserves more care than its packaging suggests. Eye protection, where appropriate, is not an upsell. It is a seatbelt.
People with darker skin tones also need a slightly more cautious approach. Visible light can produce pigmentation that lasts at least 2 weeks at certain doses. Skin of colour responds more strongly to this kind of exposure. Lower doses, careful protocols, and dermatologist input are used when the goal is to treat an existing skin condition.
Who should be more careful
Most people will be fine. A smaller group should pause and ask first. The reasons differ, but the principle is the same. The therapy is gentle, but it is not nothing. Certain skin, eye, immune system, and pregnancy conditions have different starting points.
These groups warrant extra care:
- People with darker skin tones, especially with existing pigmentation issues: Dose tolerance and pigmentation response differ. The kindest approach is conservative.
- People with photodermatoses (skin conditions triggered or worsened by light): These include solar urticaria, polymorphous light eruption, chronic actinic dermatitis, or any of the cutaneous porphyrias. A doctor’s view first.
- People taking photosensitising medication: Several common medicines make ordinary light exposure more reactive. Ask the pharmacist.
- People with autoimmune or rheumatoid conditions: The evidence here is not alarming. But light has been shown to influence immune-cell behaviour in ways that may matter where the immune system is already misfiring.
- People with a current cancer diagnosis, particularly anywhere near the treatment area: The supportive-care evidence is good, but its use sits inside a clinical setting, not a wellness shop. Talk to the oncology team.
- Pregnant women: The pelvic area and abdomen are not appropriate sites for casual light therapy in pregnancy.
- Children, particularly with eye-aimed devices: The myopia-device safety findings should give any parent pause before reaching for unmonitored use.
- Anyone using a device near the eyes: Eye protection. Always. Even if the box says you do not need it.
Red light therapy is, on balance, a gentle one. The mistake is treating “gentle” as “consequence-free at any dose, for any person, in any setting”. It is not. The same biology that makes the right dose useful makes the wrong dose pointless. A poorly chosen dose in a sensitive context can occasionally do more than waste your time.

What to Check Before Spending Money on Red Light Therapy
The aim of this final section is simple. Walk into a shop or open a website and ask a sharper question than “Is this any good?” The right question is sharper. Can this device, at this dose, do the specific thing I want, for someone like me? That sentence is the whole skill of buying red light therapy well.
The following is a working framework. Use it like a checklist. It is built on the realities we have already walked through.
- Match the wavelength to the goal.
Surface targets such as ageing skin or acne respond best to light in the deep red range. Joint, muscle and deeper-tissue targets need longer near-infrared wavelengths to reach them at all. A device that does only one type is suited only to that type of job. A device that does both has a more honest range, if the rest of its specifications hold up.
- Look at irradiance and the treated area, not the wattage.
Wattage on a box is the most marketed and least useful number. What matters is irradiance, the amount of light hitting each square centimetre, and the actual area covered. A high wattage spread over a huge mat may be feeble per centimetre. A more modest output focused on a smaller area can be appropriate. The product should disclose both. If it does not, treat that as information.
- Treatment time and distance are not optional details.
The same device at a 5 cm distance is not the same as at 30 cm. The same session length, used twice as often, is not the same protocol. Studied clinical results came from defined sessions at defined distances. The instructions on the box are not garnish.
- Look for direct testing of this device for this claim.
A clinical laser study uses a precise wavelength and dose on a defined condition. That is not evidence for a different consumer device aimed at a different goal. Borrowed evidence is not evidence. If a brand cites studies, check whether those studies used something resembling what they are selling.
- Check the safety basics.
A CE or UKCA mark is the entry-level requirement, not the trophy. Eye protection, where the device is anywhere near the eyes, is not optional. Manufacturer guidance on session length and frequency exists for a reason. Do not double up sessions to “speed it up”. The biology does not work that way.
- Plan for repetition, not for instant transformation.
Studied protocols are usually repeated sessions across weeks or months. Red light therapy rewards consistency. It does not reward intensity. People who expect a single session to deliver a noticeable change tend to walk away disappointed. They blame the technology when the expectation was the problem.
- Calibrate the size of the result you should expect.
The honest reading of the evidence is that, where they exist, the effects are moderate. Skin looks slightly fresher. Joint pain is reduced by a meaningful but not magical amount. Hair regrowth is real but gradual. Post-surgical recovery moves a little quicker. None of these is a transformation. All of them are worth having for the right person, for the right job, at the right price.
- Match the tool to the problem honestly.
For deep tissue at a distance, your home device may not have the punch. For surface skin, it might be perfectly suited. For brain or eye-related claims, a wellness panel is almost certainly out of its depth. It is being asked to do work it was not designed for. If the goal is medical, the right setting is a clinical one.
The closing thought belongs to the reader, not the device. The buyer who walks in with this checklist asks better questions than most marketing teams are prepared for. That, more than any single specification, is what protects the wallet and the body.
The light is real. The biology is real. The sales copy is sometimes ahead of both. The reader equipped to tell those three apart spends their money well. Or keeps it.
Sources
- Agostinis P, Berg K, Cengel KA, Foster TH, Girotti AW, Gollnick SO, Hahn SM, Hamblin MR, Juzeniene A, Kessel D, et al. Photodynamic Therapy of Cancer: An Update. CA Cancer J Clin. 2011;61:250-281.
- Avci P, Gupta A, Sadasivam M, Vecchio D, Pam Z, Pam N, Hamblin MR. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013 Mar;32(1):41-52.
- Avci P, Gupta GK, Clark J, Wikonkal N, Hamblin MR. Low-level laser (light) therapy (LLLT) for treatment of hair loss. Lasers Surg Med. 2014;46(2):144-151.
- Bathini M, Raghushaker CR, Mahato KK. The molecular mechanisms of action of photobiomodulation against neurodegenerative diseases: A systematic review. Cell Mol Neurobiol. 2022;42:955-71.
- Bensadoun R-J, Bollet MA, Liem X, Cao K, Magné N. New photobiomodulation device for prevention and cure of radiotherapy-induced oral mucositis and dermatitis: results of the prospective safe PBM study. Support Care Cancer. 2022;30:1569-77.
- Burton B, Parodi MB, Jürgens I, Zanlonghi X, Hornan D, Roider J, et al. LIGHTSITE II randomized multicenter trial: evaluation of multiwavelength photobiomodulation in Non-exudative Age-Related macular degeneration. Ophthalmol Ther. 2023;12:953-68.
- Cassano P, Caldieraro MA, Norton R, Mischoulon D, Trinh NH, Nyer M, et al. Reported side effects, weight and blood pressure, after repeated sessions of transcranial photobiomodulation. Photobiomodul Photomed Laser Surg. 2019;37:651-6.
- Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet. 2009;374:1897-1908.
- Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012 Feb;40(2):516-533.
- Cohen M, Austin E, Masub N, Kurtti A, George C, Jagdeo J. Home-Based Devices in Dermatology: A Systematic Review of Safety and Efficacy. Arch Dermatol Res. 2022;314:239-246.
- de Freitas LF, Hamblin MR. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J Sel Top Quantum Electron. 2016;22:7000417.
- DE Oliveira MF, Johnson DS, Demchak T, Tomazoni SS, Leal-Junior EC. Low-intensity LASER and LED (photobiomodulation therapy) for pain control of the most common musculoskeletal conditions. Eur J Phys Rehabil Med. 2022 Apr;58(2):282-289.
- da Silva MM, Albertini R, de Tarso Camillo de Carvalho P, Leal-Junior EC, Bussadori SK, Vieira SS, et al. Randomized, blinded, controlled trial on effectiveness of photobiomodulation therapy and exercise training in the fibromyalgia treatment. Lasers Med Sci 2018;33:343-51.
- European Commission. Are LED Lights Safe for Human Health?
- Ferraresi C, Kaippert B, Avci P, Huang Y-Y, de Sousa MVP, Bagnato VS, Parizotto NA, Hamblin MR. Low-level Laser (Light) Therapy Increases Mitochondrial Membrane Potential and ATP Synthesis in C2C12 Myotubes with a Peak Response at 3-6 h. Photochem Photobiol. 2015;91(2):411-416.
- Flores LJF, de Souza Campos F, Baumann L, Weber MG, Barazetti LK, Nampo FK, et al. Photobiomodulation does not improve anaerobic performance in well-trained cyclists. Lasers Med Sci. 2023;38:134.
- Glass GE. Photobiomodulation: The Clinical Applications of Low-Level Light Therapy. Aesthetic Surg J. 2021;41:723-738.
- Glass GE. Photobiomodulation: A Systematic Review of the Oncologic Safety of Low-Level Light Therapy for Aesthetic Skin Rejuvenation. Aesthetic Surg J. 2023;43:NP357-NP371.
- Hadad H, Santos AFP, de Jesus LK, Poli PP, Mariano RC, Theodoro LH, et al. Photobiomodulation therapy improves postoperative pain and edema in third molar surgeries: A Randomized, Comparative, Double-Blind, and prospective clinical trial. J Oral Maxillofac Surg. 2022;80:37e1.
- Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochemistry and photobiology. 2018;94(2):199-212.
- Hamblin MR. Photobiomodulation or Low-level Laser Therapy. J Biophotonics. 2016;9:1122-1124.
- Hashmi JT, Huang YY, Sharma SK, Kurup DB, De Taboada L, Carroll JD, Hamblin MR. Effect of pulsing in low-level light therapy. Lasers Surg Med. 2010;42:450-466.
- Hauck M, Schardong J, Donini G, Normann TC, Plentz RDM. Effects of photobiomodulation therapy (PBMT) over endothelial function in healthy individuals: a preliminary crossover clinical trial. Lasers Med Sci. 2023;38:104.
- Heiskanen V, Hamblin MR. Correction: Photobiomodulation: Lasers vs. Light Emitting Diodes? Photochem Photobiol Sci. 2019;18:259.
- Heiskanen V, Hamblin MR. Photobiomodulation: Lasers vs. Light emitting diodes? Photochem Photobiol Sci. 2018;17:1003-17.
- Huang YY, Sharma SK, Carroll J, Hamblin MR. Biphasic Dose Response in Low Level Light Therapy – An Update. Dose-Response. 2011;9(4):602-618.
- Iosifescu DV, Norton RJ, Tural U, Mischoulon D, Collins K, McDonald E, et al. Very low-level transcranial photobiomodulation for major depressive disorder: The elated-3 multicenter, randomized, sham-controlled trial. J Clin Psychiatry. 2022;83:21m14226.
- Jagdeo JR, Adams LE, Brody NI, Siegel DM. Transcranial red and near infrared light transmission in a cadaveric model. PLoS One. 2012;7:e47460.
- Jagdeo J, Nguyen JK, Ho D, Wang EB, Austin E, Mamalis A, Kaur R, Kraeva E, Schulman JM, Li C-S, et al. Safety of Light Emitting Diode-Red Light on Human Skin: Two Randomized Controlled Trials. J Biophotonics. 2020;13:e201960014.
- Jenkins PA, Carroll JD. How to Report Low-Level Laser Therapy (LLLT)/Photomedicine Dose and Beam Parameters in Clinical and Laboratory Studies. Photomed Laser Surg. 2011;29(12):785-787.
- Jiménez-García AM, Zorzo C, Gutiérrez-Menéndez A, Arias JL, Arias N. Transabdominal photobiomodulation applications: A systematic review and meta-analysis. Obes Rev. 2025 Aug;26(8):e13921.
- Karu TI. Multiple roles of cytochrome c oxidase in mammalian cells under action of red and IR-A radiation. IUBMB Life. 2010;62(8):607-610.
- Karu TI, Kolyakov SF. Exact action spectra for cellular responses relevant to phototherapy. Photomed Laser Surg. 2005;23:355-361.
- Kashiwagi S, Morita A, Yokomizo S, Ogawa E, Komai E, Huang PL, et al. Photobiomodulation and nitric oxide signaling. Nitric Oxide. 2023;130:58-68.
- Kwon HH, Lee JB, Yoon JY, Park SY, Ryu HH, Park BM, Kim YJ, Suh DH. The Clinical and Histological Effect of Home-Use, Combination Blue-Red LED Phototherapy for Mild-to-Moderate Acne Vulgaris in Korean Patients: A Double-Blind, Randomized Controlled Trial. Br J Dermatol. 2013;168:1088-1094.
- Lane N. Cell biology: power games. Nature. 2006 Oct 26;443(7114):901-903.
- Lapchak PA, Boitano PD, Butte PV, Fisher DJ, Hölscher T, Ley EJ, et al. Transcranial near-infrared laser transmission (NILT) profiles (800 nm): Systematic comparison in four common research species. PLoS One. 2015;10:e0127580.
- Leavitt M, Charles G, Heyman E, Michaels D. HairMax LaserComb laser phototherapy device in the treatment of male androgenetic alopecia: a randomized, double-blind, sham device-controlled, multicentre trial. Clin Drug Invest. 2009;29:283-292.
- Liu H, Yang Y, Guo J, Peng J, Zhao P. Retinal Damage After Repeated Low-level Red-Light Laser Exposure. JAMA Ophthalmol. 2023;141(7):693-5.
- Machado AF, Leal-Junior ECP, Batista NP, Espinoza RMCPP, Hidalgo RBR, Carvalho FA, Micheletti JK, Vanderlei FM, Pastre CM. Photobiomodulation therapy applied during an exercise-training program does not promote additional effects in trained individuals: A randomized placebo-controlled trial. Braz J Phys Ther. 2022;26:100388.
- Maghfour J, Ozog DM, Mineroff J, Jagdeo J, Kohli I, Lim HW. Photobiomodulation CME Part I: Overview and Mechanism of Action. J Am Acad Dermatol. 2024:S0190962224001865.
- Mahmoud BH, Ruvolo E, Hexsel CL, et al. Impact of long-wavelength UVA and visible light on melanocompetent skin. J Invest Dermatol. 2010;130(8):2092-2097.
- Mester E, Spiry T, Szende B, Tota JG. Effect of laser rays on wound healing. Am J Surg. 1971;122:532-535.
- Mineroff J, Maghfour J, Ozog DD, Lim HW, Kohli I, Jagdeo J. Photobiomodulation CME Part II: Clinical Applications in Dermatology. J Am Acad Dermatol. 2024:S0190962224001877.
- Mineroff J, Austin E, Jagdeo J. Cutaneous Effects of Photobiomodulation with 1072 Nm Light. Arch Dermatol Res. 2022;315:1481-1486.
- Mota LR, Duarte IDS, Galache TR, Pretti KMDS, Neto OC, Motta LJ, Horliana ACRT, Silva DDFTD, Pavani C. Photobiomodulation Reduces Periocular Wrinkle Volume by 30%: A Randomized Controlled Trial. Photobiomodulation Photomed Laser Surg. 2023;41:48-56.
- Naterstad IF, Joensen J, Bjordal JM, Couppé C, Lopes-Martins RAB, Stausholm MB. Efficacy of low-level laser therapy in patients with lower extremity tendinopathy or plantar fasciitis: systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2022 Sep 28;12(9):e059479.
- Ostrin LA, Schill AW. Red light instruments for myopia exceed safety limits. Ophthalmic Physiol Opt. 2024 Mar;44(2):241-248.
- Pinto HD, Vanin AA, Miranda EF, Tomazoni SS, Johnson DS, Albuquerque-Pontes GM, Aleixo IO Junior, Grandinetti VD, Casalechi HL, de Carvalho PT, Leal EC Junior. Photobiomodulation therapy (PBMT) improves performance and accelerates recovery of high-level Rugby players in field test: A randomized, crossover, double-blind, placebo-controlled clinical study. J Strength Cond Res. 2016.
- Pinto NC, de Ferreira MVP, Braga NL, Aldred NA, Gomes A. Customized photobiomodulation modulates pain and alters thermography pattern in patients with knee osteoarthritis: A randomized Double-Blind pilot study. Photobiomodul Photomed Laser Surg. 2022;40:698-707.
- Robijns J, Lodewijckx J, Claes S, Van Bever L, Pannekoeke L, Censabella S, Bussé L, Colson D, Kaminski I, Broux V, et al. Photobiomodulation Therapy for the Prevention of Acute Radiation Dermatitis in Head and Neck Cancer Patients (DERMISHEAD Trial). Radiother Oncol. 2021;158:268-275.
- Schmidt TR, Mármora BC, Brochado FT, Gonçalves L, Campos PS, Lamers ML, et al. Red light-emitting diode on skin healing: an in vitro and in vivo experimental study. Bras Dermatol. 2025;100:54-62.
- Stausholm MB, Naterstad IF, Joensen J, Lopes-Martins RÁ, Sæbø H, Lund H, et al. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open 2019;9:e031142.
- Tomazoni SS, Almeida MO, Bjordal JM, Stausholm MB, Machado CD, Leal-Junior EC, et al. Photobiomodulation therapy does not decrease pain and disability in people with non-specific low back pain: a systematic review. J Physiother 2020;66:155-65.
- Valverde A, Hamilton C, Moro C, Billeres M, Magistretti P, Mitrofanis J. Lights at night: does photobiomodulation improve sleep? Neural Regen Res.
- Wunsch A, Matuschka K. A Controlled Trial to Determine the Efficacy of Red and Near-Infrared Light Treatment in Patient Satisfaction, Reduction of Fine Lines, Wrinkles, Skin Roughness, and Intradermal Collagen Density Increase. Photomed Laser Surg. 2014;32:93-100.
- Ye H, Xiang Y. Clinical efficacy of 830 Nm LED photobiomodulation therapy on postoperative blepharoplasty complications. Aesthetic Plast Surg. 2025;49:655-63.
- Zein R, Selting W, Hamblin MR. Review of light parameters and photobiomodulation efficacy: dive into complexity. J Biomed Opt. 2018 Dec;23(12):1-17.
- Zhang R, Qu J. The mechanisms and efficacy of photobiomodulation therapy for arthritis: A comprehensive review. Int J Mol Sci. 2023;24:14293.

{kind=link}