

Tight hip flexors affect millions globally, limiting movement and contributing to numerous health issues. According to research, hip mobility restrictions are among the most common flexibility issues reported across diverse populations. This prevalence highlights hip mobility’s importance for everyday function and overall well-being.
The hip joint represents one of the body’s most complex structures. It can move in multiple directions through a complex system of muscles, tendons, and ligaments. Central to hip function are the hip flexors, a group of muscles responsible for bringing the thigh toward the torso.
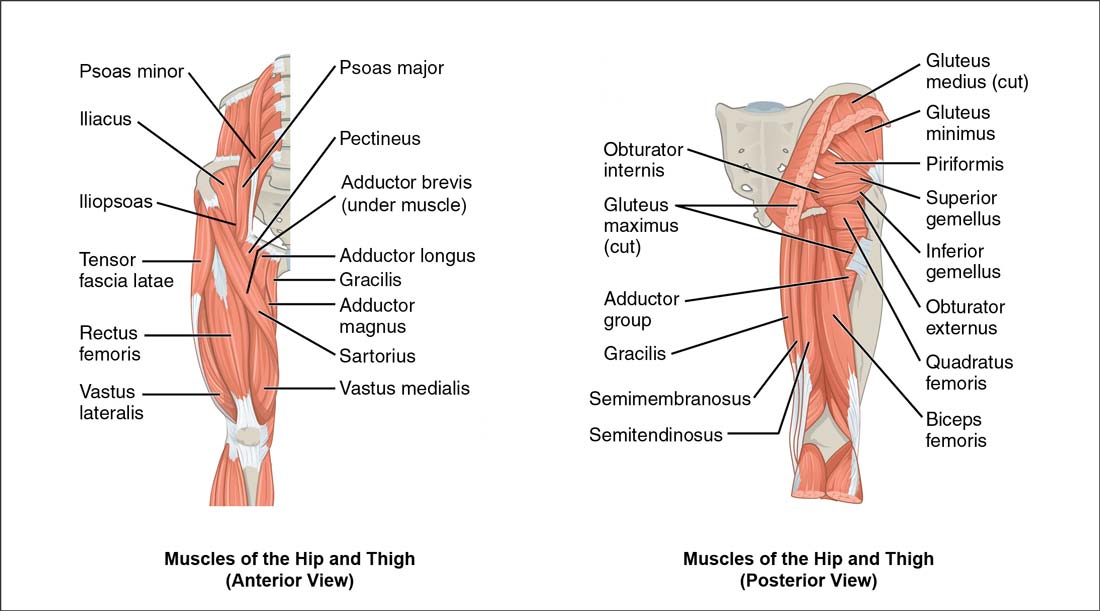
These muscles include the iliopsoas (comprising the psoas major and iliacus), rectus femoris, sartorius, and tensor fasciae latae (TFL). See the image below for a detailed anatomical view. Each plays a vital role in walking, running, sitting, and maintaining proper posture.
What makes hip flexor tightness particularly insidious (gradually developing in a harmful way) is how it develops without obvious symptoms until significant restriction has occurred. For most people, especially those with desk jobs, hip flexors remain in a shortened position for hours daily.
Eventually, these muscles adapt to this inactive, compressed state. This adaptation becomes your body’s new “normal,” resulting in reduced flexibility, strength, and overall hip mobility that can trigger a cascade of compensatory problems.
The reduction in hip mobility doesn’t exist in isolation—it creates a chain reaction throughout your kinetic chain. Your body consists of interconnected systems; when one area becomes restricted, others must compensate.
Limitation in tight hip flexors frequently leads to excessive lumbar extension, anterior pelvic tilt (forward tilt of the pelvis), hamstring overactivation, and gluteal weakness. These compensations can manifest as lower back pain, knee discomfort, postural abnormalities, and headaches.
While understanding flexibility limits and the distinction between muscle tension and structural compression is essential for addressing any mobility restriction, hip flexor tightness presents unique challenges requiring specific assessment and targeted interventions.
Like hamstring flexibility, hip flexor mobility involves complex anatomical relationships influencing your entire movement system.
Throughout this article, we’ll explore the impact of hip tightness on your health and fitness, examine quick tests to assess your current hip mobility and provide evidence-based solutions to improve function.
From understanding the anatomical relationships to learning practical stretching techniques and preventative strategies, you’ll discover how addressing this common restriction can unlock improved performance and reduce pain.
Understanding Tight Hip Flexors and Their Anatomy
The complexity of hip function becomes apparent when considering that approximately 17 muscles contribute to hip joint movement. As shown in the anatomical illustration above, these muscles work together in coordinated control patterns. Each muscle serves multiple functions, creating an advanced system of movement and stability.
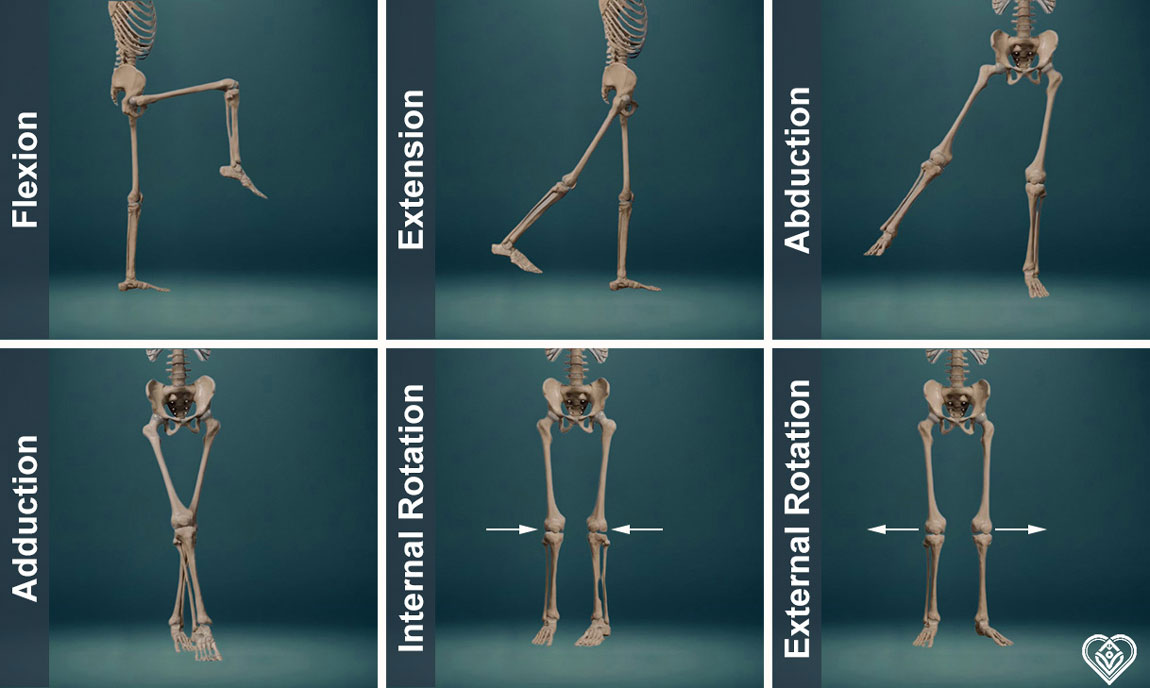
The hip joint’s extensive mobility comes from its ball-and-socket design, allowing for movement in multiple planes. This joint achieves its range through six fundamental movement patterns, clearly demonstrated in the skeletal illustrations above. These movements shape how tight hip flexors impact overall mobility.
Let’s examine each primary hip movement pattern:
- Flexion: Moving your thigh forward and upward toward your torso, with a normal range of 90-135 degrees
- Extension: Taking your leg backwards away from your body’s midline, typically ranging from 10-30 degrees
- Abduction: Lifting your leg sideways away from your body’s centre, with a normal range of 30-50 degrees
- Adduction: Drawing your leg inward toward or across your body’s midline, typically 10-30 degrees
- Internal Rotation: Rotating your thigh inward toward your body’s centre, ranging from 30-45 degrees
- External Rotation: Turning your thigh outward away from your body’s midline, normally 45-60 degrees
- Combined Movements: These basic patterns frequently merge, creating complex movement combinations essential for daily activities and athletic performance
The precise nature of hip mobility becomes evident when examining the role of tight hip flexors in movement limitations. The iliopsoas complex, from the lumbar spine to the femur, is a significant stabiliser bridging the spine, pelvis, and leg. This comprehensive anatomical positioning explains why hip flexor issues can trigger widespread movement compensations.
Research demonstrates that the psoas major is crucial in lumbar stability due to its unique anatomical position and function. Biomechanical (relating to the mechanical laws of body movement) models reveal that they provide spinal stiffness and act like supporting guy wires to alleviate spine stress during lifting activities. This stabilising function proves essential for maintaining proper posture and preventing injury.
The central nervous system carefully orchestrates these muscular relationships, selecting optimal activation patterns to balance spine loading and stability. When hip flexor function becomes compromised, it alters the contribution of antagonist (opposing) and supporting trunk muscles to spine stability. This neural adaptation explains why addressing hip mobility requires a comprehensive understanding of these anatomical relationships.
Research shows that the iliopsoas generate significant compression force on the lumbar spine, contributing substantially to spinal stability. While this compression is necessary for proper function, it can become problematic when hip flexors remain chronically tight. The altered movement patterns can lead to excessive joint stress and compensatory movements throughout the kinetic chain.
Common Causes of Hip Flexor Tightness in Modern Life
The prevalence of tight hip flexors has risen dramatically with modern lifestyle changes. Research indicates that sedentary behaviour significantly reduces hip extension flexibility, with studies showing that approximately two-thirds of investigated populations have limited hip extension mobility. This widespread issue affects those who already experience symptoms and those unaware of developing restrictions.
Our bodies adapt to the positions we maintain throughout the day. For most people in contemporary society, this means prolonged periods of sitting – at desks, in cars, on sofas. When we sit, our hip flexors remain in a shortened position. Over time, these muscles adapt to this compressed state, gradually losing their natural length and flexibility.
Prolonged Sitting
The impact of extended sitting reaches beyond straightforward muscle shortening. Studies reveal daily sitting for more than 8 hours leads to measurable muscle length and function changes. Office workers show significant alterations in muscle activation patterns and postural alignment.
Additionally, different sitting positions create varying levels of muscle imbalance. Crossing legs for more than three hours daily leads to asymmetrical hip positioning. This uneven stress distribution affects the hip flexors and creates compensatory patterns throughout the kinetic chain.
Poor Postural Habits
How we sit proves as necessary as how long we sit. Many people unconsciously adopt positions that exacerbate tight hip flexors. Slouching, leaning to one side, or sitting with the pelvis tucked under all contribute to muscle imbalances.

Occupational Demands
Modern work environments often require repetitive movements or sustained positions that stress the hip flexors:
- Prolonged standing in one position
- Repetitive bending and lifting
- Regular kneeling or squatting
- Extended periods of driving
- Frequent stair climbing
Studies indicate these activities contribute significantly to hip flexor restrictions without proper movement variation.
High-Heeled Footwear
For many women, regular use of high heels creates additional stress on hip flexors. The altered biomechanics force the body to adapt its positioning, particularly affecting the iliopsoas and rectus femoris muscles. This mechanical alteration shifts weight distribution and creates lasting postural changes.
Rapid Growth Periods
Physical development, particularly during adolescence, can contribute to hip flexor tightness. Rapid skeletal growth and increasingly sedentary lifestyles create an environment where muscle imbalances readily develop. The restriction in spine mobility during these periods often compounds hip flexor issues.
Stress Response
Physical tension from psychological stress significantly impacts muscle function. The body’s fight-or-flight response triggers muscle guarding, particularly in core stabilising muscles. Many people unknowingly hold tension in their hip flexors during periods of stress, creating chronic patterns of tightness.
Exercise Patterns
Even active individuals can develop hip flexor issues through imbalanced training approaches. Excessive focus on specific exercises while neglecting others can create muscle imbalances. For instance, runners and cyclists often develop tight hip flexors due to the repetitive nature of their sports without adequate counterbalancing movements.
How Tight Hip Flexors Affect Your Back and Overall Health
The impact of tight hip flexors is not limited to simple mobility restrictions. Research reveals that 50-80% of people experience low back pain, with hip mobility limitations playing a significant role in this prevalence. This connection stems from the biomechanical relationship between hip function and spinal health.
People with non-specific low back pain typically show approximately 10° less hip passive range of motion than those without pain. This reduced mobility creates a chain of compensatory movements. When the hip extension becomes limited, the lower back must move excessively to achieve standard movement patterns.
Postural Changes
Limited hip extension forces the pelvis to tilt forward excessively. This anterior pelvic tilt (forward tilt of the pelvis) creates an exaggerated curve in the lower back. Moreover, studies show that people with tight hip flexors often develop muscle imbalances throughout their core region.
The body attempts to stabilise these postural changes by activating other muscles inappropriately. Research indicates that this compensation leads to:
- Overactive lower back muscles
- Weakened abdominal muscles
- Reduced gluteal strength
- Hamstring tension
- Altered movement patterns
Movement Compensation
The relationship between hip mobility and functional movement proves particularly significant in athletic performance. Female athletes with restricted hip extension show notably reduced gluteus maximus activation and altered muscle coordination patterns. This change in muscle recruitment can lead to:
- Increased stress on knee joints
- Higher risk of a hamstring strain
- Reduced power output
- Compromised running mechanics
- Balance difficulties
Balance and Stability
Research demonstrates that hip flexor tightness correlates strongly with reduced dynamic balance performance. This balance impairment increases fall risk and affects athletic performance across various sports. The connection lies in how hip mobility affects weight distribution and the body’s ability to respond to movement challenges.
Cardiovascular Impact
Surprisingly, research links hip mobility to cardiovascular health. Studies show poor trunk flexibility is associated with arterial stiffening, a recognised risk factor for cardiovascular disease. Regular stretching improves vascular function through increased blood flow and reduced arterial stiffness.

Nerve Function
Hip flexor tension can affect nerve pathways running through the hip region. The psoas muscle borders critical neural structures, and chronic tension in this area may create subtle patterns of nerve compression. This can present as:
- Radiating discomfort
- Altered sensation patterns
- Referred pain
- Movement hesitation
- Muscle guarding
Sports Performance
Athletes with hip flexor restrictions often develop compensatory movement patterns that compromise performance. Research shows that football players with tight hip flexors experience greater activation of certain muscle groups, leading to premature fatigue and increased injury risk.
Daily Function
Even simple daily activities become affected by hip flexor restrictions. Research indicates that limited hip extension can alter:
- Walking patterns
- Stair climbing ability
- Sitting comfort
- Standing posture
- Sleep quality
Long-term Implications
Chronic hip flexor tightness creates lasting changes in spinal positioning. Studies reveal that sustained postural alterations can lead to:
- Disc pressure changes
- Facet joint stress
- Muscle length adaptations
- Movement pattern alterations
- Chronic pain development
Assessing Hip Flexor Mobility with the Thomas Test
Before addressing tight hip flexors, you need a way to assess your current mobility. The Thomas Test offers a simple yet effective method for checking hip flexor flexibility at home. This test helps identify which specific hip flexor muscles might need attention.
The beauty of this assessment lies in its simplicity – you only need a sturdy table or kitchen counter. The surface should be slightly elevated, allowing your legs to hang freely without touching the floor. This positioning ensures accurate results by letting gravity act naturally on your leg position.
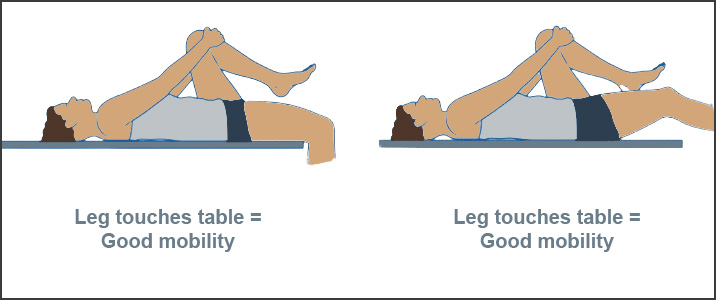
As illustrated above, you’ll make two key observations when performing the test. First, check if the back of your thigh touches the surface – this simple checkpoint immediately reveals your hip flexor mobility status. Second, notice the degree of knee bend – ideally around 80 degrees. These visual indicators, clearly shown in the illustration, tell you about different aspects of hip flexor mobility.
Steps to Perform the Thomas Test:
- Find a sturdy, elevated surface that allows your legs to dangle
- Sit on the edge of the surface
- Gently lie back while drawing both knees toward your chest
- Hold one leg firmly against your chest
- Slowly lower the other leg, letting it relax completely
- Observe the position of your lowered leg
What Your Results Mean:
- Good Mobility: Back of thigh touches the surface with knee bent about 80 degrees
- Limited Mobility: The thigh doesn’t touch the surface
- Muscle-Specific Tightness: Knee straightens significantly while thigh touches the surface
For best results, perform this test after a brief warm-up before any strenuous activity. Test both sides to identify differences between your right and left hip flexors. This information proves valuable when addressing mobility restrictions.
Effective Stretching Techniques for Tight Hip Flexors
Addressing tight hip flexors requires a systematic approach to stretching. Research demonstrates that properly executed stretching, particularly following evidence-based protocols, can significantly improve hip extension range of motion.
Moreover, unlike other muscle groups where excessive stretching might impair performance, hip flexors respond positively to appropriate stretching durations.
Start with a kneeling lunge position, ensuring one knee rests on the ground while the other foot plants forward. The crucial element many people miss involves correctly positioning your pelvis. Actively tuck your tailbone under and engage your gluteal muscles (muscles in your buttocks). This action flattens the front of the hip and provides proper stretch to the hip flexors rather than merely arching your lower back.
Reach your arm upward on the same side as the kneeling leg for deeper release. Gently bend toward the opposite side while maintaining the tucked pelvis position. Research shows that this combination of movements activates the posterior chain (back of body muscles) more effectively while stretching the hip flexors, enhancing overall effectiveness.
Another practical approach starts from a seated position with feet hip-width apart and hands slightly behind your shoulders. Lift your hips and step one foot back onto the ball of the foot. Again, the pelvis position proves crucial – engage your core muscles and posteriorly tilt your pelvis while pointing your knee away until you feel the stretch through the front of the hip.
Studies comparing different stretching techniques reveal that dynamic and proprioceptive neuromuscular facilitation (PNF) methods improve mobility. The PNF approach involves contracting the stretched muscle before relaxing into a deeper stretch, creating beneficial changes in muscle tissue and nervous system function.
Consistency proves more valuable than intensity when implementing these stretches for tight hip flexors. Research supports performing stretches twice daily, morning and evening, for approximately 15 minutes. This moderate but regular approach allows for gradual tissue adaptation without overwhelming recovery capacity.
Hold each position for 30 seconds, followed by a 10-second relaxation period. Perform two sets on each side, alternating between legs. This timing protocol has shown optimal results in research studies, promoting flexibility gains while avoiding diminishing returns that can occur with excessive durations.
For maximum benefit, consider these evidence-based guidelines:
- Warm up gently before stretching
- Maintain steady breathing throughout
- Avoid bouncing or forcing movements
- Progress gradually with intensity
- Listen to your body’s response
- Maintain proper pelvic position
- Focus on quality over quantity

Long-Term Strategies to Maintain Healthy Hip Flexors
Preventing tight hip flexors requires thoughtful integration of movement into daily life. Research shows that maintaining muscle flexibility stems from regular, mindful attention rather than sporadic, intense efforts. Small, consistent changes in daily habits create lasting improvements in hip mobility.
Motion therapy has demonstrated significant benefits for hip mobility. Several clinical studies highlight its therapeutic potential, particularly when incorporated into daily activities. Simple movement breaks during prolonged sitting periods help maintain hip flexor length and function.
Strengthening core muscles effectively supports hip flexor health. Research indicates that proper abdominal and gluteal strength helps maintain optimal pelvic positioning, reducing stress on hip flexors. This balanced approach prevents overcompensation patterns from developing.
Implementing a progressive exercise programme proves particularly effective. Starting with gentle movements and gradually increasing intensity allows tissues to adapt appropriately. This measured approach builds sustainable mobility while respecting the body’s natural adaptation processes.
Ergonomics plays a vital role for office workers. Studies show that maintaining good posture during work hours significantly impacts hip flexor health. Regular position changes, proper chair height, and occasional standing periods improve hip mobility.
Exposure to varied movement patterns enhances long-term mobility. Research demonstrates that incorporating different types of motion improves motor control and leads to higher levels of coordinated muscle activation. This variety prevents the development of restrictive movement patterns.
Tight hip flexors respond particularly well to consistent attention. Evidence suggests that regular mobility routines create lasting muscle length and function changes. Morning mobility practices often prove incredibly beneficial, setting a positive tone for daily movement patterns.
Combining stretching, strengthening, and movement awareness creates comprehensive hip health. Research shows that this integrated approach yields better long-term results than focusing solely on flexibility. Regular assessment helps track progress and adjust strategies as needed.
A well-balanced lifestyle naturally supports hip mobility. While stretching and exercise play crucial roles, factors like proper hydration, adequate sleep, and stress management influence muscle health and flexibility. Research indicates that these lifestyle elements significantly impact tissue quality and recovery capacity.
Movement represents our natural state—our bodies flourish with regular, varied motion. Consistent attention to hip mobility supports our hip flexors and overall capacity for comfortable, efficient movement throughout life.
Sources
- Arampatzis A, Laube G, Schroll A, Frank J, Bohm S, Mersmann F. Perturbation-based exercise for prevention of low-back pain in adolescent athletes. Transl Sports Med. Published online 2021.
- Aslan H, Buddhadev HH, Suprak DN, San Juan JG. Acute Effects Of Two Hip Flexor Stretching Techniques On Knee Joint Position Sense And Balance. Int J Sports Phys Ther. 2018 Aug;13(5):846-859. Erratum in: Int J Sports Phys Ther. 2019 Apr;14(2):173.
- Bisconti AV, Cè E, Longo S, Venturelli M, Coratella G, Limonta E, Doria C, Rampichini S, Esposito F. Evidence for improved systemic and local vascular function after long-term passive static stretching training of the musculoskeletal system. J Physiol. 2020;598:3645–66.
- Bogduk N, Pearcy M, Hadfield G. Anatomy and biomechanics of psoas major. Clin Biomech. 1992;7:109–119.
- Brown SHM, Potvin JR. Constraining spine stability levels in an optimisation model leads to the prediction of trunk muscle co-activity and improved predictions of spine compression. J Biomech. 2005;38:745–754.
- Carlson C. Axial back pain in the athlete: Pathophysiology and approach to rehabilitation. Curr Rev Musculoskelet Med. 2009;2(2):88-93.
- Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech. 1996;11:1–15.
- Clapis PA, Davis SM, Davis RO. Reliability of inclinometer and goniometric measurements of hip extension flexibility using the modified Thomas test. Physiother Theory Pract 2008; 24: 135–41.
- Das S, Sarkar B, Sharma R, Mondal M, Kumar P. Prevalence of lower cross syndrome in young adults: a cross sectional study. Int J Adv Res. 2017;5:2217–2228.
- Endo Y Sakamoto M. Relationship between lower extremity tightness and star excursion balance test performance in junior high school baseball players. J Phys Ther Sci. 2014;26(5):661-663.
- Fatoye F, Gebrye T, Odeyemi I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol Int 2019; 39: 619-26.
- GBD 2013 mortality and causes of death collaborators Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385:117–71.
- Godges JJ, Macrae H, Longdon C, Tinberg C, Macrae PG. The effects of two stretching procedures on hip range of motion and gait economy. J Orthop Sports Phys Ther. 1989;10(9):350-357.
- González-de-la-Flor Á, García-Pérez-de-Sevilla G, Domínguez-Balmaseda D, del-Blanco-Muñiz JÁ. Validity and reliability of a new hip flexor muscles flexibility assessment tool: the reactive hip flexor (RHF) test. Phys Ther Sport. 2023;64:41–7.
- Hatefi M, Babakhani F, Ashrafizadeh M. The effect of static stretching exercises on hip range of motion, pain, and disability in patients with non-specific low back pain. J Exp Orthop. 2021 Jul 27;8(1):55.
- Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci Sports Exerc. 1998;30:301–310.
- Kim WD, Shin DC. Correlations between hip extension range of motion, hip extension asymmetry, and compensatory lumbar movement in patients with non-specific chronic low back pain. Med Sci Monit. 2020;26:e925080–e925081.
- Konrad A, Močnik R, Titze S, Nakamura M, Tilp M. The influence of stretching the hip flexor muscles on performance parameters. A systematic review with meta-analysis. Int J Environ Res Public Health. 2021;18:1–20.
- Marieb E. N. Hoehn K. Human anatomy and physiology. 10th ed. San Francisco, CA: Pearson Benjamin Cummings; 2015.
- Mendiguchia J., Alentorn-Geli E., Idoate F., Myer G.D. Rectus Femoris Muscle Injuries in Football: A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies. Br. J. Sports Med. 2013;47:359–366.
- Mettler J.H., Shapiro R., Pohl M.B. Effects of a Hip Flexor Stretching Program on Running Kinematics in Individuals With Limited Passive Hip Extension. J. Strength Cond. Res. 2019;33:3338–3344.
- Mills M., Frank B., Goto S., Blackburn T., Cates S., Clark M., Aguilar A., Fava N., Padua D. Effect of Restricted Hip Flexor Muscle Length on Hip Extensor Muscle Activity and Lower Extremity Biomechanics in College-Aged Female Soccer Players. Int. J. Sports Phys. Ther. 2015;10:946–954.
- Nishiwaki M, Yonemura H, Kurobe K, Matsumoto N. Four weeks of regular static stretching reduces arterial stiffness in middle-aged men. Springerplus. 2015;4:555.
- Pannell SL. Logan university. Vol. 13. Chesterfield (MO): Logan University; 2012. The postural and biomechanical effects of high heel shoes: a literature review; pp. 1–23.
- Park Y, Bae Y. Comparison of postures according to sitting time with the leg crossed. J Phys Ther Sci. 2014;26:1749–1752.
- Peterson Kendall F, Kendall McCreary E, Geise Provance P, McIntyre Rodgers M, Anthony Romani W (2005) Muscles Testing and Function with Posture and Pain. 5th ed. Baltimore: Lippincott Williams & Wilkins.
- Puagprakong P, Kanjanasilanont A, Sornkaew K, Brady W. The effects of lower crossed syndrome on upper body posture during sitting in female office workers. Muscle Ligaments Tendons J. 2022;12:621–627.
- Rahman A, Adon M, Shahar H. Association between awkward posture and musculoskeletal disorders among assembly line workers in an automotive industry. January 2014Malaysian Journal of Medicine and Health Sciences 10(10):23-28.
- Roach SM, San Juan JG, Suprak DN, Lyda M, Bies AJ, Boydston CR. Passive hip range of motion is reduced in active subjects with chronic low back pain compared to controls. Int J Sports Phys Ther. 2015;10:13–20.
- Roach S, San Juan JG, Suprak DN, Lyda M. Concurrent validity of digital inclinometer and universal goniometer in assessing passive hip mobility in healthy subjects. Int J Sports Phys Ther. 2013;8:680–688.
- Santaguida PL, McGill SM. The psoas major muscle: A three-dimensional geometric study. J Biomech. 1995;28:339–345.
- Silfies SP, Mehta R, Smith SS, Karduna AR. Differences in feedforward trunk muscle activity in subgroups of patients with mechanical low back pain. Arch Phys Med Rehabil. 2009;90:1159–1169.
- Stokes IA, Gardner-Morse MG, Henry SM. Abdominal muscle activation increases lumbar spinal stability. Clin Biomech (Bristol, Avon) 2011;26:797–803.
- Sung PS. Multifidi muscles median frequency before and after spinal stabilisation exercises. Arch Phys Med Rehabil. 2003;84:1313–1318.
- Winters MV, Blake CG, Trost JS, Marcello-Brinker TB, Lowe L, Garber MB, Wainner RS. Passive versus active stretching of hip flexor muscles in subjects with limited hip extension: A randomised clinical trial. Phys Ther. 2004;84:800–807.
- Yamamoto K, Kawano H, Gando Y, Iemitsu M, Murakami H, Sanada K, Tanimoto M, Ohmori Y, Higuchi M, Tabata I, Miyachi M. Poor trunk flexibility is associated with arterial stiffening. Am J Physiol Heart Circ Physiol. 2009;297:H1314–8.

{kind=link}